
30 years of LASIK





Thirty years ago, in the summer of 1989, the U.S. Patent and Trademark Office granted a patent to a retinal surgeon Gholam Peyman, MD, for a “Method for Modifying Corneal Curvature.”1
The method came to be known as laser in-situ keratomileusis (LASIK). The patent represented a major landmark in evolution of eye care. It was the culmination of more than a century of innovations in science and technology.
It also coincided with the start of a transformative practice model-the collective engagement of optometrists and ophthalmologists in the care of a patient.
Eye care has come a long way since the summer of ’89. Correcting sphere and cylinder is no longer enough. Eyecare practitioners have advanced to treating higher order aberrations we couldn’t even detect thirty years ago.
Related: Epi-on cross-linking may speed recovery
We now expect vision outcomes better than 20/20 for the majority of our patients.
Today, both optometrists and ophthalmologists are advancing the field of spectacle independence. From prevention to treatment of refractive error, ODs and MDs are united by a common goal to help our patients lead healthy and productive lives.
More than 100 years ago, Hermann Snellen introduced the concept of surgically altering cornea to reduce refractive error.2 Initially, refractive surgery developed along two paths-radial keratotomy (RK) and lamellar surgery, called keratomileusis.3 The invention of excimer laser in the early ‘80s made RK obsolete and transformed keratomileusis into the LASIK of today.
The initial years of excimer laser work brought together scientists and clinicians with diverse backgrounds and expertise.
Related: How to determine an ideal LASIK candidate
Initially, a trio of IBM scientists discovered an ability of the newly invented excimer laser to accurately reshape biological tissue without damage to the surrounding tissue. The connection between the laser and the eyes was made by Stephen Trokel, MD.4
Thousands of plastic test blocks, cadaver eyes, and animal eyes later, the first laser vision correction, photorefractive keratectomy (PRK), was performed on a sighted eye in 1988.
A year later, Gholam Peyman, MD, patented a method that combined excimer laser of the ‘80s and keratomileusis of the ‘60s into the procedure that became known as LASIK.


Since then, more than 40 million LASIK procedures have been performed worldwide with success rates of 99.5 percent as measured by visual acuity and patient satisfaction.5
A recent collaborative study among the U.S. Food & Drug Administration (FDA), the National Eye Institute (NEI), and the Department of Defense confirmed the high rate of patient satisfaction after LASIK.6
Related: How to manage vision changes over time post-LASIK
LASIK has come a long way
The first LASIK procedure was performed in 1990. It was FDA approved in 1999. The year 2019 marks a double anniversary for LASIK-30 years since it was patented and 20 years since it was FDA approved.
In the initial years of LASIK, advancements were focused on fine-tuning the accuracy of correcting refractive error-myopia, astigmatism, and hyperopia. In the early 2000s, attention was turned to improving LASIK safety with the introduction of the femtosecond laser, which replaced the mechanical microkeratome for LASIK flap creation.
Subsequent work in LASIK vision correction has been directed at improving procedure customization to achieve correction of both refractive error and higher-order aberrations, aiming for the goal of improving day and night quality of vision, and achieving vision beyond 20/20 for most patients.
The customization of LASIK began in the mid-2000s with the advent of wavefront-guided ablations.
Related: Managing LASIK complications
Initially, 200 data points were measured and attempts were made to reduce the aberrations. Over the past 15 years with the evolution of customization technology, precise detection and


mapping of aberrations has become possible.
Three custom LASIK systems are currently available:
Modern wavefront-guided LASIK (iDesign Advanced Wave Scan, Johnson & Johnson Vision) targets 1,200 aberration data points in the optical system
Wavefront-optimized LASIK (Wavelight, Alcon) uses laser beam application techniques that optimize corneal asphericity to maintain good quality of vision day and night
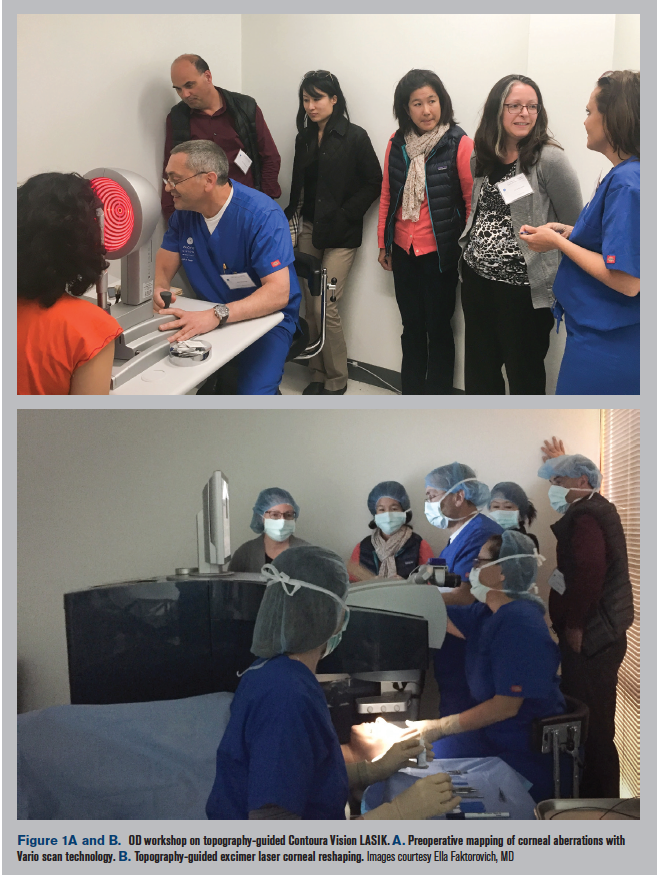
Topography-guided LASIK (Contoura Vision, Wavelight, Alcon) aims at correcting corneal aberrations by mapping 22,000 elevation and depression points on the corneal surface
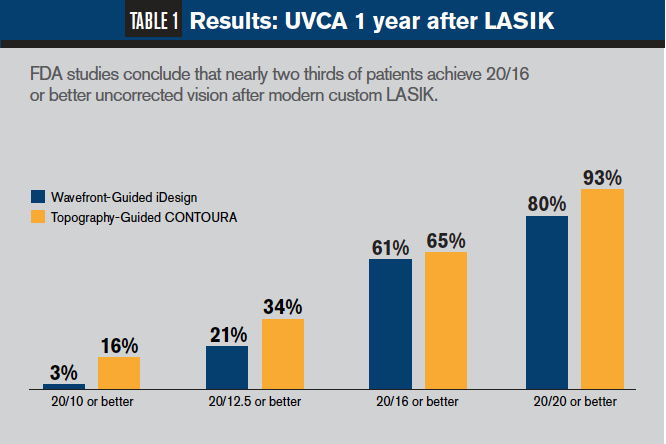
With custom LASIK, eyecare practitioners can offer patients better vision than ever. For example, in the recent FDA studies of topography-guided Contoura Vision LASIK and wavefront-guided iDesign LASIK, nearly two thirds of patients achieved better than 20/16 uncorrected vision.7
Today, “better than 20/20” is the new 20/20.
As LASIK evolved, so did the relationship between optometrists and ophthalmologists. Proper patient selection, counseling, and thorough pre- and post-LASIK exams are as crucial to successful outcomes as surgical skill, nomograms, and laser technology.
Related: Quality of life after LASIK
The role of the optometrist
Optometrists are the leaders in diagnosing ametropias. At the conclusion of an eye exam, the optometrist will inevitably discuss ametropia correction. In a post-teenage young adult with a healthy ocular system and clear natural lens, glasses, contact lenses (both soft and gas permeable lenses), and refractive surgery should all be considered.
For patients, LASIK is the noun that loosely, albeit incorrectly, is used to cover all refractive surgeries, including PRK, small incision lenticular extraction (SMILE), implantable collamer lens (ICL), and refractive lens exchange (RLE).
In pre-op management, optometry’s first role is to educate the patient about refractive surgery options and counsel the patient about the procedure(s) he may benefit from the most.
Related: Why I changed what I tell patients about refractive surgery
The optometrist is also well positioned to leverage her long-term relationship with the patient to determine what procedure will best fit the patient’s lifestyle and vision needs.
If LASIK is the best choice, the OD can communicate to the surgeon whether full distance, monovision, or undercorrection OU will be best as well as the post-op refractive goal.
The initial surgery work-up in the modern optometric office can supply the patient with a near total representation of LASIK candidacy:
Refraction: Both dry (non-cycloplegic) and wet (cycloplegic) will provide a baseline numerical starting point to guide the laser treatment. The wet refraction will aid in preventing over-minusing. Based on refraction alone, the optometrist can counsel the patient whether he is within the range for laser vision correction, including LASIK, or whether ICL or RLE would be better.
Slit-lamp exam: This will help to define any abnormal anterior segment pathology. Slit lamp combined with corneal staining (sodium fluorescein and lissamine green) is a great way to assess dry eye. In the presence of dry eye, aggressively starting treatment can pave the way for successful and accurate laser refractive surgery.
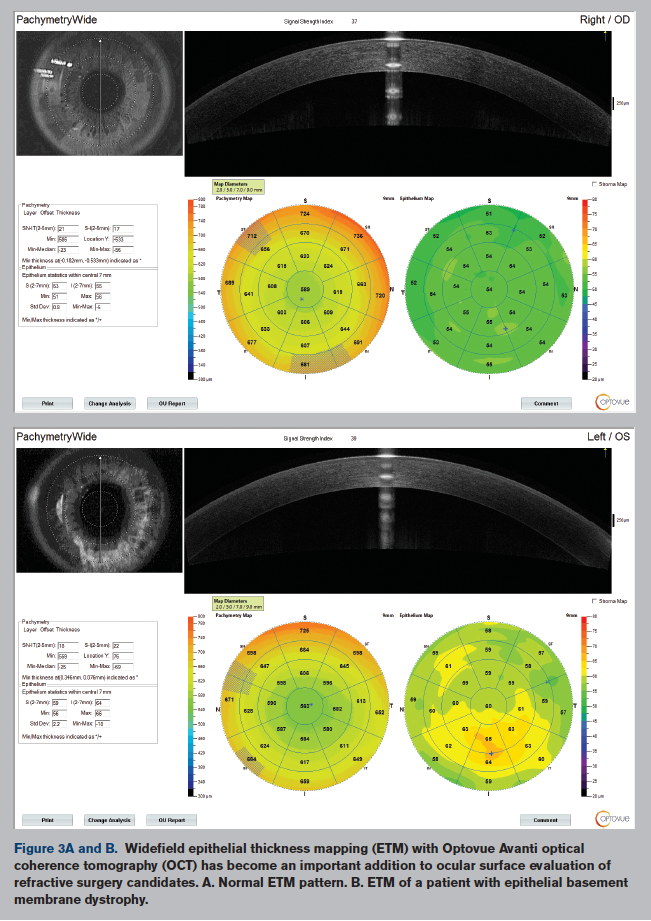
In the time period between the optometrist’s visit and refractive surgery evaluation, dry eye can be successfully managed. Today, there are many options for successful dry eye management before and after LASIK. Epithelial basement membrane dystrophy and significant corneal scars detected on slit-lamp exam would steer the patient toward PRK rather than LASIK.
Corneal topography/tomography: Such imaging is an important tool in assessing corneal shape and symmetry as a screener for ectasia risk. If a topography/tomography is unavailable, measuring keratometry (K) values with an automated device or manual keratometer will provide the Ks and show the quality of the mires.
Pachymetry: This measurement is also a useful guideline because it will help guide tissue ablation abilities for corneal laser surgery.
Related: Technology helps to diagnose corneal ectasia
Advances in dry eye management improve healing after LASIK


Optometrists are well-equipped to assess and manage patients during their post-LASIK follow-ups.
The most common finding during the first several months after LASIK is dryness, which can be successfully managed with effective treatment options.
From immunomodulators such as Xiidra (lifitegrast, Novartis) that reduces inflammation and helps produce better quality tears, to the reformulated Restasis Multidose (cyclosporine, Allergan) that enhances patient compliance, to intranasal neurostimulators such at TrueTear (Allergan) that triggers patient’s own tear production, we can help our patients heal faster.
The efficacy of modern dry eye management is supported by recent research.
Related: How to treat dry eye in the pediatric and young adult population
At the 2019 American Society of Cataract and Refractive Surgery (ASCRS) meeting, a study by Schallhorn et al dispelled many dry eye myths.8 Preop dry eye did not translate to post-op dry eye, and in fact, some patients with moderate to severe dry eye experienced less ocular surface disease symptoms after LASIK.
The results of the Patient-Reported Outcomes with LASIK (PROWL) studies launched by the FDA, the National Eye Institute, and the Department of Defense have also concluded that with modern pre- and post-LASIK dry eye management patients experience excellent outcomes.
These studies revealed that in most patients, preoperative dry eye symptoms decreased after LASIK. Even though some patients experienced new dry eye symptoms at three months, these were categorized as mild and improved with time and ocular surface management.6
Related: Overlooked causes of dry eye
What’s next?
Advances in surgical customization are likely to continue with more patients able to achieve vision beyond 20/20.
The SMILE procedure is promising, but it needs to incorporate treatment of higher-order aberrations to achieve the same level of customization as modern LASIK surgery.
The concept of presbyLASIK may continue to be explored to improve both distance and near vision in presbyopic patients while minimizing side effects of a multifocal cornea.
Novel therapeutic approaches to stimulating corneal nerve regeneration and restoring corneal nerve function and sensitivity are being investigated. Nerve growth factor, Cenegermin-containing eye drops (Oxervate, Dompé) have been FDA approved for the treatment of neurotrophic keratitis. Further investigation could help determine if such types of medications could enhance healing after LASIK.
We have come a long way in the past 30 years.
Read more cornea content here
Disclosures:
1. Free Patents Online. Method for Modifying Corneal Curvature. Available at: http://www.freepatentsonline.com/4840175.pdf. Accessed 10/7/19.
2. McAlinden C. Corneal refractive surgery: past to present. Clin Exp Optom. 2012 Jul;95(4):386-98.
3. Reinstein DZ, Archer TJ, Gobbe M. The history of LASIK. J Refract Surg. 2012 Apr;28(4):291-8.
4. Bloomberg Business. LASIK Surgery: How IBM’s Dr. James Wynne Discovered It. Available at: https://www.youtube.com/. Accessed 10/7/19.watch?v=yzavwVLefPw
5. Sandoval HP, Donnenfeld ED, Kohnen T, Lindstrom RL, Potvin R, Tremblay DM, Solomon KD. Modern laser in situ keratomileusis outcomes. J Cataract Refract Surg. 2016 Aug;42(8):1224-34.
6. Eydelman M, Hilmantel G, Tarver ME, Hofmeister EM, May J, Hammel K, Hays RD, Ferris F 3rd. Symptoms and Satisfaction of Patients in the Patient-Reported Outcomes With Laser In Situ Keratomileusis (PROWL) Studies. JAMA Ophthalmol. 2017 Jan 1;135(1):13-22.
7. Moshirfar M, Shah TJ, Skanchy DF, Linn SH, Kang P, Durrie DS. Comparison and analysis of FDA reported visual outcomes of the three latest platforms for LASIK: wavefront guided Visx iDesign, topography guided WaveLight Allegro Contoura, and topography guided Nidek EC-5000 CATz. Clin Ophthalmol. 2017 Jan 4;11:135-147.
8. Schallhorn J. Challenging conventional wisdom about LASIK. Presented at: American Society of Cataract and Refractive Surgery annual meeting; May 3-7, 2019; San Diego.
9. Optical Society of America. How a leftover Thanksgiving dinner gave us LASIK surgery. Available at: https://phys.org/news/2013-11-leftover-thanksgiving-dinner-gave-lasik.html. Accessed 10/7/19.











Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.
















