
Go beyond medical treatment for recurrent corneal erosion




A healthy corneal epithelium is fundamental to healthy vision, and several corneal epithelial diseases are associated with severe consequences to overall ocular health.1,2
Recurrent corneal erosion (RCE), which is characterized by a disturbance at the level of the corneal epithelial basement membrane and results in defective adhesions and recurrent breakdowns of the epithelium, is a primary culprit.3
RCE is never a one-and-done occurrence. The name says it all. Until an appropriate and effective treatment is implemented, the patient can expect recurrent breakdown of the corneal epithelium.
Optometrists’ goal in treating patients with RCE is to determine the best way to regenerate or repair the epithelial basement membrane to restore the bond between the epithelium and the anterior stroma and thereby put a stop to the destructive cycle and associated pain.
Related: Use amniotic membrane in the primary care officeSigns and symptoms
RCE typically announces itself with sudden onset of pain that may last from minutes to several hours. In the most severe cases, which include persistent epithelial defects, patients can experience pain for several days.3 Associated symptoms of RCE include redness, photophobia, blurred vision, and tearing.4
A detailed slit lamp examination should be performed with fluorescein staining and retro-illumination.5 Slit-lamp findings include conjunctival injection, fresh or healing epithelial defects, and/or epithelial basement membrane dystrophy (EBMD).
If the RCE episode is recent, optometrists should see no evidence of corneal infection. If, on the other hand, the patient has had several episodes of RCE, a corneal scar may be present.6Related: Visual haze leads to diagnosing unknown corneal dystrophy
While RCE typically presents as a unilateral condition, there are instances when both eyes may exhibit EBMD.6
Ocular pain is typically the motivating factor that prompts patients to seek help from their eyecare providers.
Once the patient is in my care, I reassure him that there are effective treatment options; then I take a detailed history so I can begin gathering the building blocks that will put me on the path to identifying the best strategy to manage his condition.
The two primary therapeutic goals are to facilitate rapid re-epithelialization and relieve ocular pain; a secondary goal is to prevent future occurrences of erosion.
Related: How pain gates affect dry eye and chronic pain Causes and consequences
A thorough patient history will almost always reveal that patients who present with RCE have had a corneal abrasion, EBMD, a corneal dystrophy, or prior ocular surgery.
The highest rates of RCE occur in patients who also have dry eye disease (DED), diabetes mellitus, blepharitis, and ocular rosacea.
RCE results from mechanical trauma to the superficial cornea, with about 45 percent to 64 percent of reported cases being related to prior physical injury. The second most common cause is EBMD, which has been reported in 19 percent to 29 percent of cases.5Related: Avoiding the pitfall of epithelial basement membrane dystrophy


RCE differential diagnosis should include:
Herpes simplex virus (HSV)
Epithelial keratitis
Exposure keratopathy
Neurotrophic keratitis
Conjunctival foreign body
DED
Infectious keratitis
Ocular graft-versus-host disease (GVHD)
Chemical and thermal burns
Floppy eyelid syndrome
Salzmann’s nodular degeneration
A weak attachment between the epithelium and the basement membrane-thought to be related to the epithelial adhesion network and associated filament-characterizes RCE.


Patients who are at higher risk for developing RCE have higher levels of matrix metalloproteinases (MMP)-9 and Interleukin 1 (IL-1) in the tears, and studies show that patients with RCE have increased activity of MMP-2 and MMP-9.6,7
These enzymes can adversely affect the basement membrane and anchoring fibrils, thereby causing dysfunctional adhesion complexes.7,8
These factors influence my treatment choices.
Related: Amniotic membrane in ocular surface disease Treatment options
Medications such as antibiotic drops and preservative-free lubricating drops used in conjunction with nighttime lubricating or hypertonic saline ointments were historically relied upon as first-line RCE treatment.
Take note: It is never appropriate to use bland petroleum-based ointment at night time-bland petroleum ointment will soften the epithelial tissue at night and make the it susceptible to erosion.
Depending on the patient’s level of discomfort, a cycloplegic eye drop or a soft bandage contact lens might be added. Oral analgesics could also be administered if necessary.3
In my experience, traditional medical treatment almost always requires additional therapy to obtain relief from this very painful and often debilitating condition. This is among the reasons why it is so important to determine the underlying cause of the RCE.
If RCE is unilateral, a good case history will reveal whether or not trauma was involved, and a careful corneal evaluation determines if EBMD is present. This is important even if trauma was the underlying factor because the trauma may have been the exacerbating element that allowed the EMBD to turn into RCE.
It is also important for the practitioner to determine if exposure keratitis is present because a partial blink or nocturnal lagophthalmos could be an exacerbating factor that allowed the EMBD to transition into RCE.
Because of these underlying concerns, it is often necessary to go beyond medical treatment to more comprehensive interventions when managing patients with RCE.
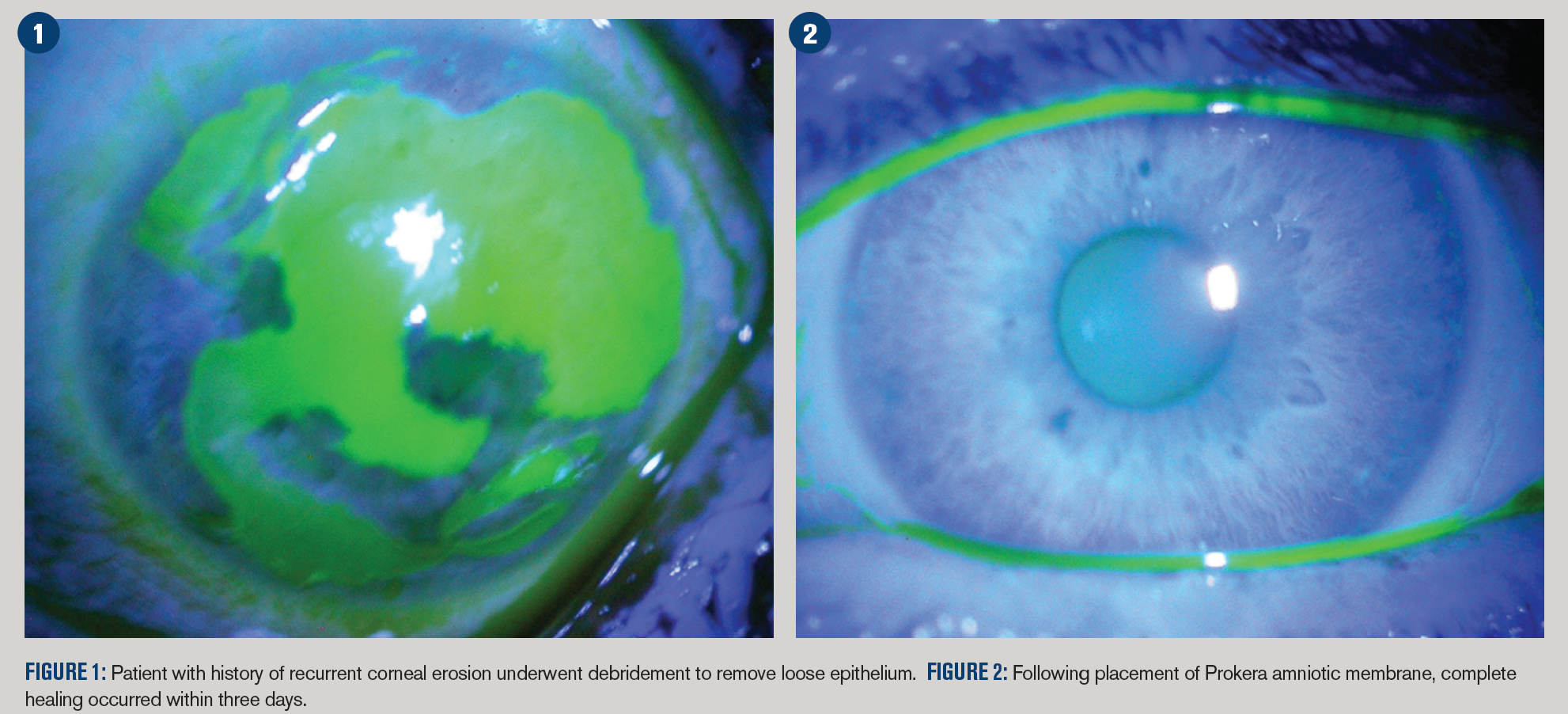
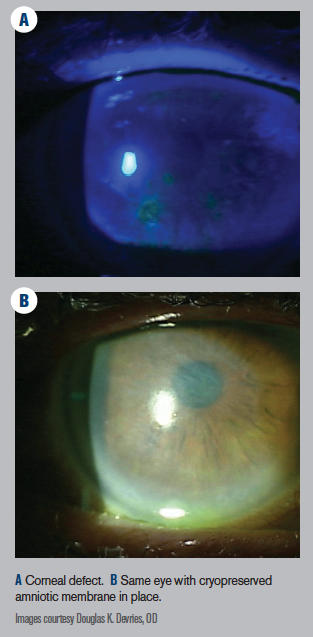
For instance, cryopreserved amniotic membrane (AM) has become a staple RCE treatment in my practice. The membrane protects the cornea from eyelid trauma while encouraging epithelial regrowth and adhesion.
Related: Amniotic membrane grafts help ocular surface disease
In one study, Huang and coworkers placed amniotic membranes onto 11 eyes of nine RCE patients, and only one eye had an RCE recurrence that required retreatment; the other 10 eyes remained asymptomatic.9
Two types of AM are available for ophthalmic use: cryopreserved and dehydrated.
Cryopreserved AM (Prokera, BioTissue) is kept frozen or refrigerated and brought to room temperature before application.
Dehydrated AM, such as AmbioDisk (IOP Ophthalmics/Katena) and BioDOptix (Integra LifeSciences) is stored at room temperature and rehydrated for clinical use.
In my clinical experience, I have found cryopreserved AM effective in managing and resolving RCE. My belief is that it is due to the anti-inflammatory properties of the biologic heavy chain-hyaluronic acid and pentraxin 3 (HC-HA/PTX3). Cryopreserved AM retains HCHA PTX3, which is the specific biologic matrix that has been identified as being responsible for AM’s anti-inflammatory and regenerative healing properties.
Related: How inflammation may play a role in retinal disease
Research also suggests that HC-HA/PTX3 helps reduce scar formation that can lead to impaired vision.10 Dehydrated AM tissue does not retain this critical biologic compound.11
Prokera cryopreserved AM is cleared and designated by the FDA for therapeutic properties, such as anti-inflammatory, protective, and wound healing effects, while dehydrated AM is not.12
Cryopreserved AM may be used to treat RCE, EBMD, persistent epithelial defects, chemical burns of the ocular surface, and corneal epithelial defects such as those associated with bullous or band keratopathy, among other conditions.
Research suggests that in addition to stimulating active healing, cryopreserved AM initiates corneal nerve regeneration.7
As noted earlier, patients with RCE often show increased levels of MMPs enzymes. These enzymes dissolve the basement membrane and its anchoring components including integrins, laminin, and type VII collagen.13
Cryopreserved AM contains inhibitors of MMPs and active matrix components including collagen type VII and laminin, essential for regenerative healing and prevention of recurrence.14
First-line use of cryopreserved AM allows for the introduction of healing properties and prevents further corneal surface deterioration.11 If the RCE has an underlying disorder of EMBD that was caused by trauma-especially recent trauma-I find the best results emerge when I use cryopreserved AM to manage the condition.
Related: Treating inflammation tackles filamentary keratitis
There are instances when it is appropriate to refer an RCE patient for a cornea consult. I refer my patient to a corneal specialist if I believe the it requires a penetrating therapeutic keratectomy.
However, even in those cases I will continue managing the patient medically because there is usually an underlying abnormality that will require monitoring and treatment to prevent reoccurrence.
In conclusion
RCE is a debilitating and painful corneal condition that can pose a serious threat to visual health. RCE may occur spontaneously or secondary to corneal injury. Patients with RCE often show increased levels of enzymes such as MMPs that dissolve the basement membrane and its anchoring components.
Cryopreserved AM is an effective RCE solution because it contains inhibitors of MMPs and active matrix components including collagen type VII and laminin, essential for regenerative healing and prevention of RCE recurrence.
Read more cornea content
References:
1. Rolando M, Zierhut M. The ocular surface and tear film and their dysfunction in dry eye disease. Surv Ophthalmol. 2001 Mar;45 Suppl 2:S203-10.
2. Katzman LR, Jeng BH. Management strategies for persistent epithelial defects of the cornea. Saudi J Ophthalmol. 2014 Jul;28(3):168-72.
3. Miller DD, Hasan SA, Simmons NL, Stewart MW. Recurrent corneal erosion: A comprehensive review. Clin Ophthalmol. 2019 Feb 11;13:325-335
4. Chen YT, Huang CW, Huang FC, Tseng SY, Tseng SH. The cleavage plane of corneal epithelial adhesion complex in traumatic recurrent corneal erosion. Mol Vis. 2006 Mar 23;12:196-204.
5. Albert DM, Jakobiec FA, Miller JW. Recurrent corneal epithelial erosion. In: Albert & Jakobiec’s Principles and Practice of Ophthalmology. Philadelphia; Edinburgh: Saunders/Elsevier; 2008.
6. Reidy JJ, Paulus MP, Gona S. Recurrent erosions of the cornea: epidemiology and treatment. Cornea. 2000 Nov;19(6):767-71.
7. Garrana RM, Zieske JD, Assouline M, Gipson IK. Matrix metalloproteinases in epithelia from human recurrent corneal erosion. Invest Ophthalmol Vis Sci. 1999 May;40(6):1266-70.
8. Sakimoto T, Shoji J, Yamada A, Sawa M. Upregulation of matrix metalloproteinase in tear fluid of patients with recurrent corneal erosion. Jpn J Ophthalmol. 2007 Sep-Oct;51(5):343-46.
9. Huang Y, Sheha H, Tseng S. Self-retained amniotic membrane for recurrent corneal erosion. J Clin Exp Ophthalmol. 2013;4(2):272.
10. Cheng AM, Zhao D, Chen R, Yin HY, Tighe S, Sheha H, Casas V, Tseng SC. Accelerated restoration of ocular surface health in dry eye disease by self-retained cryopreserved amniotic membrane. Ocul Surf. 2016 Jan;14(1):56-63.
11. Fini ME, Cook JR, Mohan R. Proteolytic mechanisms in corneal ulceration and repair. Arch Dermatol Res. 1998 Jul;290(suppl):S12-23.
12. U.S. Food & Drug Administration. Prokera 510(k) approval documents. Available at: https://www.accessdata.fda.gov/cdrh_docs/pdf3/k032104.pdf. Accessed 9/25/19.
13. Heiligenhaus A, Li HF, Yang Y, Wasmuth S, Steuhl KP, Bauer D. Transplantation of amniotic membrane in murine herpes stromal keratitis modulates matrix metalloproteinases in the cornea. Invest Ophthalmol Vis Sci. 2005 Nov;46(11):4079-85.
14. Cooke M, Tan EK, Mandrycky C, He H, O’Connell J, Tseng SC. Comparison of cryopreserved amniotic membrane and umbilical cord tissue with dehydrated amniotic membrane/chorion tissue. J Wound Care. 2014 Oct;23(10):465-74, 476.










Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.
















