
Blog: A case of Demodex infestation with eyelash extensions


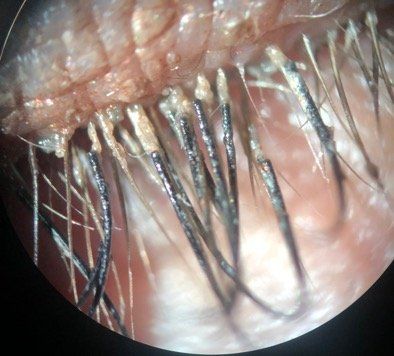
Figure 1: Demodex mites bury themselves facedown near the root of the eyelash, creating a classical cylindrical dandruff at the base of the lash follicle in patients wearing eyelash extensions.



The views expressed here belong to the author. They do not necessarily represent the views of Optometry Times or Multimedia Healthcare.
It is all too common for an asymptomatic patient to present exhibiting chronic dry eye and blepharitis signs, or for a patient to have previously been unsuccessfully treated by not having the actual cause identified.
The root of the problem may lie within the root of the eyelash follicle-an eight-legged obligate parasite.
Related: Diagnosing demodex
Case history
A 32-year-old female presented with bilateral worsening itchy eyes, intermittent blur, epiphora, and overall conjunctival injection. Upon slit-lamp examination, it was obvious this patient had false lash extensions capped on the ends of most of her upper lashes.
The patient reported she had avoided washing her eyelashes because she worried the lash extensions would be ruined. Because of this lack of hygiene, the patient created a perfect harbor for Demodex (D.) folliculorum to flourish.
Related: A different approach to treating demodex blepharitis
Parasites in the lashes
Demodex is the most common microscopic ectoparasite living on the human skin and is often present in healthy, asymptomatic individuals. These parasitic mites are opportunistic and provide positive benefits by ridding the eyelash area of waste.
But while there are different Demodex species, only D. brevis and D. folliculorum are found on humans. Demodex is most often transferred between host via contact of hair, eyebrows, and sebaceous glands on the nose.2
The rounder female Demodex mite continues the life cycle by laying 15 to 20 eggs within the hair follicle, which develop into larvae that eventually become adults in about seven days. The life cycle of an adult is usually two to three weeks.1
Previously by Dr. Coats: Blog: Recognize the signs of SND in your patients
Over their lifespan, these eight-legged mites are capable of walking approximately 8 to16 mm/hour, and are typically more active in the dark, receding into the follicle with bright light.2
Slit-lamp observation with a high magnification (25x) provides a close look to visualize the mites’ tails at the base of the eyelash follicle.
In my practice, I find that D. folliculorum and D. brevis are frequently the culprit of chronic anterior blepharitis, worsened meibomian gland disease (MGD), and lipid tear deficiency. It is thought that Demodex feeds on skin cells and sebum of the lid margin and pilosebaceous glands, causing direct damage that can trigger an inflammatory cascade.
D. folliculorum mites are about 0.4 mm in length and usually live in clusters primarily on the face. D. folliculorum is often found within the lash follicle and is more associated with disorders of the eyelashes, contributing to chronic anterior blepharitis.1
D. brevis mites tend to be shorter-about 0.2 mm in length-and live in solitary. Feeding on sebaceous gland oils D. brevis burrows deep into sebaceous and meibomian glands, and is associated with causing posterior blepharitis, meibomian gland dysfunction, and keratoconjunctivitis.1Related: How to educate patients on risks of eyelash enhancements
Signs and symptoms
Research indicates Demodex infestation can be identified by the pathognomonic cylindrical sleeve of dandruff caused by an increase in keratinization mixed with lipids.3
During infestation, several mites are typically found clustered around one follicle, creating waxy deposits that encircle the base of the eyelash. Common complaints of patients affected by D. folliculorum and D. brevis may include eyelid and eyebrow itching (especially worse in the morning), red and swollen lid margins, madarosis, chronic MGD, and chronic blepharoconjunctivitis.3
Demodex can cause direct mechanical and hypersensitivity changes to the lid margins and follicle area.1
Gently using forceps to move and stimulate the lash follicle can reveal the mechanical blockage of the glands caused by D. folliculorum. The dead mites and their excrements within the lash follicle and meibomian glands can also directly cause a hypersensitive inflammatory cascade, resulting in blepharitis and itching symptoms associated with the infestation.
Related: What's all the craze about Demodex?
Risk factors
Increasing age is one of the main risk factors for Demodex; mites are naturally found in approximately 25 percent of 20-year-olds, 84 percent of 60-year-olds, and 100 percent in patients older than age 70.1,3
Acne rosacea has also been shown to increase the risk of Demodex-associated blepharitis by creating an ideal environment for it to thrive.
According to the National Rosacea Society, patients with rosacea have approximately 18 times more D. folliculorum mites present compared with those who don’t have rosacea.4
One study indicates that with rosacea, the mean density of Demodex mites is 10.8 mites per cm2 in comparison to 0.7 mites per cm on the skin of healthy patients, increasing the risk for symptomatic infestation.2
Related: Help prevent Demodex's chronic lid and lash problems
Because of these statistics, I educate all patients with rosacea of their increased risk, encourage good lid hygiene, and recommend initiating a lid scrub regimen at bedtime.
Poor lid hygiene is also a common risk factor for Demodex, affecting both natural and false lashes. In my practice, the large majority of patients with eyelash extensions and false lashes that are not removed properly have some degree of associated D. folliculorum and/or D. brevis infestation at the base of the lash extension. (See Figure 1)
It appears that the eyelash extensions applied to individual lashes create an ideal environment for these parasites to thrive. The biggest problem patients report with lash extensions is that they are worried to wash, rinse, or clean their expensive lash extensions for fear they will come off and money will be wasted.
Related: Demodex may be beneficial to humans
Treatment
Demodex infestations require immediate attention, starting with hygiene. The goal of treatment is to alleviate symptoms by eradicating the mites and their eggs as soon as possible to prevent further mating and avoiding re-infestation.
An in-office procedure such as BlephEx (Rysurg)- a handheld device with a micrograde scrubbing sponge-can be used to help mechanically remove debris from the base of the lashes.
I also demonstrate how and where to properly clean the eyelash base and lid margin with lid scrubs. Once the patient understands they have crawling mites within their lashes, compliance is not an issue.
Because D. brevis has an affinity for oil-based cosmetics, mascara and lipid-based eye makeups should be discarded and restarted only after successful management of the infestation.
To help clean other areas of the head and face, a tear-free baby shampoo with tea tree oil (TTO) as an ingredient is recommended. Although 100 percent TTO can be irritating and should be diluted for optimal use, Cliradex (Bio-Tissue, Inc.) Towelettes containing TTO have proven effective in eradicating infestation at the base of the lash.1
Related: The role of lid hygeine in ocular surface disease
An antibiotic/steroid ointment such as Tobradex (tobramycin and dexamethasone, Alcon) can also help to slow mite movement, and possibly suffocate them. The combination steroid offers an additional benefit to reduce secondary inflammation associated with the leftover dead mites.
Some rosacea patients may also be comanaged by their dermatologist, who may also recommend oral ivermectin (Stromectol, Merck & Co., Inc.), an anti-parasitic shown to be effective in treatment of anterior blepharitis associated with D. folliculorum.4
Symptomatic patients are thoroughly educated that without proper lid hygiene, chronic blepharitis and dry eye disease will continue to be a concern with or without lash extensions.
Conclusion
The risk of Demodex infestation increases with age, acne rosacea, and poor lid hygiene-including unmaintained eyelash extensions. No matter what initial treatment is chosen, it is important for patients to understand that this is a chronic condition requiring ongoing care and maintenance.
Although D. folliculorum and D. brevis can affect real and false lashes, lash extensions seem to create a more ideal environment conducive for Demodex to flourish. Correctly identifying the root cause of a patient’s chronic dry eye disease and blepharitis is important in successfully treating Demodex living in the eyelashes.
Read more blogs here
References:
1. Liu J, Sheha H, Tseng SC. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010;10(5):505-10.
2. Rather PA, Hassan I. Human demodex mite: the versatile mite of dermatological. Indian J Dermatol. 2014 Jan;59(1):60-6.
3. Post CF, Juhlin E. Demodex folliculorum and blepharitis. Arch Dermatol. 1963 Sep;88(3):298–302.
4. Jarmuda S, O’Reilly N, Zaba R, Jakubowicz O, Szkaradkiewicz A, Kavanagh K. Potential role of Demodex mites and bacteria in the induction of rosacea. J Med Microbiol. 2012 Nov;61(11):1504-1510.
Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.












 of patients believe that medical technology innovations will enhance care for the aging population, with 90% of providers recognizing the need to address specific requirements for older patients. Image credit: AdobeStock/buritora")




