
Branded vs generics: You make the call


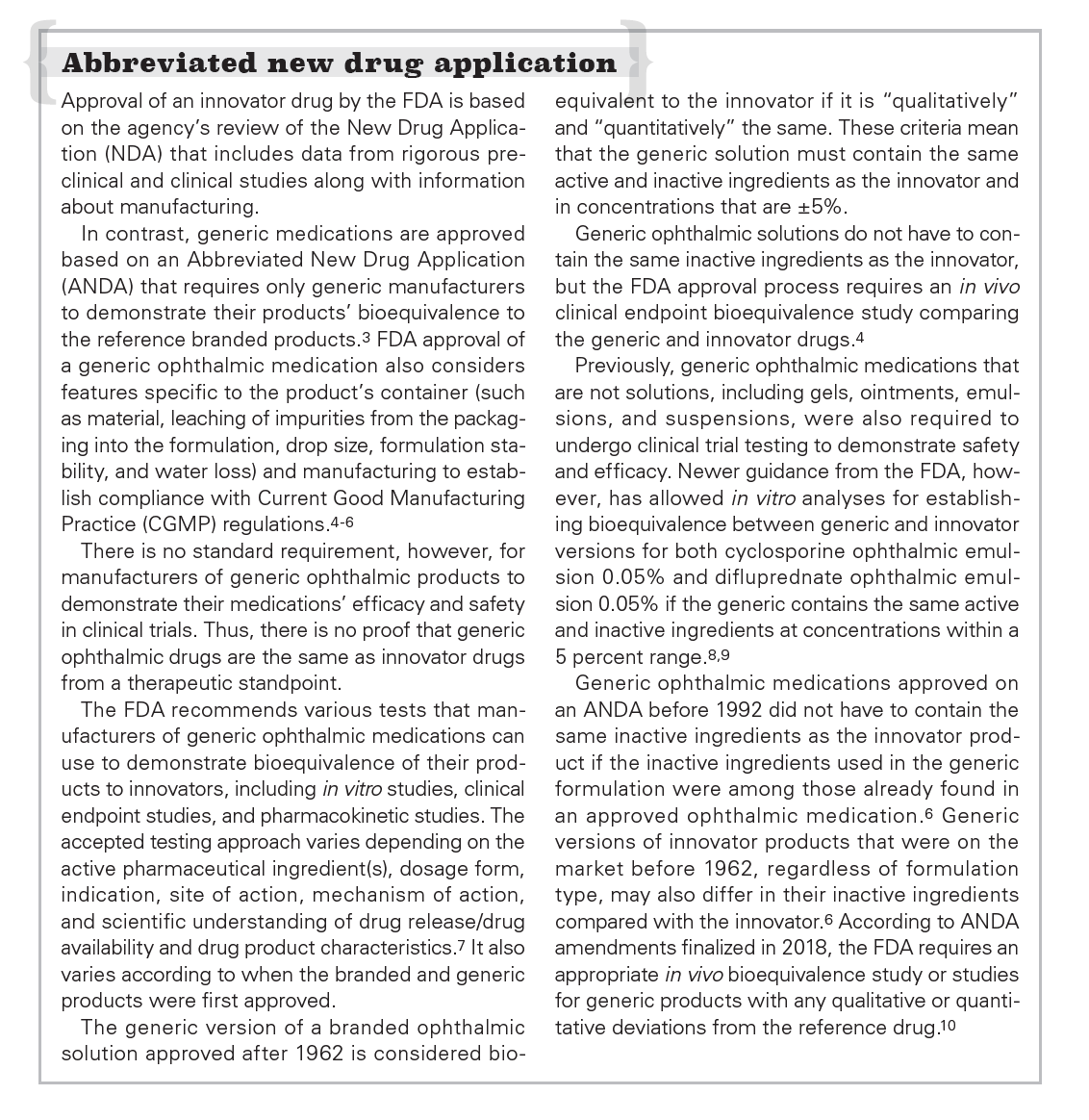
Sidebar: Abbreviated New Drug Application


Disclosures:
Dr. Mangan receives consulting fees from Shire Pharmaceuticals.
Dr. Bowling receives speaking and consulting fees from Alcon Laboratories and Shire Pharmaceuticals
Rising healthcare expenditures have focused attention on increasing the use of generic medications as a way to help control costs. Data on dispensed prescriptions show that in 2016, 89 percent of dispensed retail prescriptions were accounted for by generic medications.1 Controversy, however, surrounds the drive to go generic.
In a recent study, investigators analyzing Medicare Part D data found that eyecare providers were responsible for a higher percentage of branded medication claims than all other providers.2
As discussed by key opinion leaders in this supplement, the finding is understandable considering the host of concerns that clinicians will factor into decisions when they need to make the call between generic and branded medications.
Basis for branded preferences
Optometrists dedicated to optimizing patient outcomes say that greater confidence in the efficacy, safety, and tolerability of branded medications is a key reason why they favor the branded product when there is a generic alternative.
This trust in innovator formulations and uncertainty about the clinical performance of generic products originates partly from knowledge about the different pathways generic and branded ophthalmic medications follow to gain U.S. Food & Drug Administration (FDA) approval (see sidebar:
Abbreviated New Drug Application).3-10
Impressions about the benefits of branded medications and concerns about generics are supported by findings of published studies and reinforced by personal clinical experience. The advantages available from using branded drugs that have no generic alternatives along with the higher-than-expected cost of some generic medications further underlie prescribing patterns favoring branded ophthalmic drugs.
Ernie Bowling, OD, MS, FAAO, FNAP, in Gadsden, AL, and editor emeritus of Optometry Times, says that while the FDA requires manufacturers of generic medications to demonstrate their products’ bioequivalence to the branded product, determining bioequivalence for topical ophthalmic medications may be based on pharmaceutical equivalence rather than clinical pharmacokinetics studies. Furthermore, manufacturers of generic ophthalmic medications do not need to conduct clinical trials to establish the safety and effectiveness of their products.
“I am confident and comfortable using branded medications that have undergone rigorous development and testing, but I don’t know what patients will be getting with a generic medication,”he says. “The only consistent feature between branded and generic ophthalmic medications is the identity of the active ingredient.”
Richard B. Mangan, OD, FAAO, is assistant professor and member of the clinical faculty for the department of ophthalmology, University of Colorado School of Medicine in Aurora, CO. He says that because of the different regulatory requirements for approval of generic medications, there is room for significant differences in the formulations of branded medications and generic versions and therefore in the clinical performance of these product types.
“Variations allowed in the inactive ingredients in generic products can greatly influence pH, tonicity, buffering capacity, and viscosity,” he says. “Considering variability in packaging characteristics that determine drop size and the ease with which patients can dispense the medication introduces concern about whether the appropriate dose is consistently delivered.”
Reviewing the evidence on equivalence
Inactive ingredients constitute the major portion of ophthalmic medications. For example, excipients account for 99.995% of the contents in a bottle of latanoprost 0.005% (Xalatan, Pfizer) ophthalmic solution. Findings from analytical studies show how the permitted differences in type of inactive ingredients and their concentration can translate into physicochemical differences between generic and branded medications, which can mean differences in efficacy, safety, and tolerability.
For instance, studies that compared the innovator latanoprost product with generic versions identified differences in specific gravity, osmolarity, pH, buffer capacity, and viscosity.11-13 In addition, analyses showed some generic latanoprost products contained more particulate matter than the branded product and were more prone to active ingredient degradation when exposed to temperature conditions that may be encountered in routine use.12 The research also showed that some generics contained concentrations of the active ingredient that exceeded compendial limits.11
Drop size was also reported to be larger for generic medications compared with branded latanoprost.11,13 Commenting on the clinical relevance of this finding, researchers noted that larger drop size along with higher active ingredient concentration in the generic latanoprost product could lead to more systemic absorption; more local side effects, including conjunctival hyperemia, iris pigmentation, and eyelash lengthening; as well as increased risk of cystoid macular edema and uveitis in patients at risk for these prostaglandin-associated complications.11
Similarly, investigators comparing branded â¨timolol maleate ophthalmic gel forming solution â¨(Timoptic-XE, Bausch + Lomb) with generic equivalents found significant variation between the two product groups in viscosity, surface tension, and bottle tip design. Drop volume also differed significantly with the branded medication delivering a significantly smaller drop volume than a generic.14
“A larger drop size has potential safety ramifications and can also result in the need for an earlier refill, which means patients will be spending more money, especially if the refill interval is so short that it is not covered by insurance,” he says.
Dr. Mangan says manufacturers of branded ophthalmic medications dedicate significant resources to bottle design, giving careful attention to drop size and ease of dispensing.
“Any cost saving from using a generic versus a branded medication may be lost if the drop size is larger with the generic or more medication is lost because of handling difficulty leading to inaccurate delivery,” he says.
Says Dr. Bowling: “I have patients telling me that they are unable to get a drop out of the bottle of a particular generic intraocular pressure (IOP)-lowering medication because the container is so hard to squeeze.”
This anecodotal observation is confirmed by a laboratory analysis. Evaluating the containers of the branded latanoprost and generic products included in their study, Kolko et al reported differences in the average force needed to dispense the medication, with the branded medication requiring the least pressure.13
Kolko et al also observed variation in bottle shape and cap color among the five generic products they analyzed.13 The differences in product appearance are remarkable considering that cap color is the feature that patients use most to identify their medications.15 With no guarantee that patients will be dispensed a generic from the same manufacturer at each prescription refill, lack of uniformity in medication cap color may lead to confusion and problems with proper drug administration.
“I explain to patients that generic versions of a given medication can be manufactured by multiple companies, and so there is the potential for product variation with each refill,” Dr. Bowling says. “With the change they may find a difference in product appearance, ease of handling, or drop size, and the inconsistency can create confusion that can lead to medication errors or noncompliance.”
There is a paucity of clinical studies comparing outcomes associated with use of generic versus branded ophthalmic medications.2 The available studies have generated inconsistent findings, but they also vary in methodological quality.
A recent retrospective cohort study analyzing medical claims data for patients with primary open-angle glaucoma concluded that the generic latanoprost was no less effective and possibly more effective than branded prostaglandins for preventing the need for additional medication or surgery.16
In contrast, prospective, comparative clinical trials reported differences between generic and branded latanoprost that favor the branded medication.
A randomized, parallel study compared the efficacy and safety of two generic latanoprost solutions and the branded product in 60 patients with treatment-naïve open-angle glaucoma.17 After 16 weeks, IOP was significantly reduced from baseline in all three groups, and there were no treatment-related differences in the percentage reduction in IOP. Safety evaluations, including analyses of changes in tear breakup time and the Ocular Surface Disease Index supported better ocular surface safety in the group using branded latanoprost.
In a crossover, masked, three-month study, researchers found no significant changes in diurnal IOP values after patients with open-angle glaucoma were switched from branded latanoprost to a generic version.18 Tolerability was also similar for the two products. Nevertheless, the branded product was associated with a significantly greater number of IOP reductions below 14 mm Hg compared with the generic, which the investigators noted may be clinically significant considering evidence that progression from moderate to advanced glaucoma can be limited by a target IOP lower than 14 mm Hg.
Significantly greater IOP-lowering using the branded product versus a generic was also documented in a study investigating timolol maleate 0.5% gel-forming solution.19
A section on generic IOP-lowering medications in the European Glaucoma Society’s Terminology and Guidelines for Glaucoma notes that the similarity in efficacy and tolerability of generic and branded medications is not well studied.20 Citing reports showing variable clinical results, differences in drop size, number of drops, bottle structure, and tip configuration, along with the development of corneal epithelial disorders associated with generic products, the guidelines recommend that IOP be closely monitored when switching patients from branded to generic drugs.


In a study evaluating patients who were switched from branded to generic latanoprost, investigators administered a questionnaire to obtain users’ perspectives regarding a variety of practical concers.21 The collected data showed that 75 percent of patients preferred the brand name latanoprost. Overall, patients found the branded product easier to open and instill as well as more comfortable when administered. Furthermore, 20 percent of patients noted that their generic medications failed to last a month as expected. Written comments showed that with generic medications, drops dispensed in multiples or ran down the face.
Clinical experiences
Dr. Bowling says that the problems he sees in patients using generic medications for IOP-lowering relate more to ocular surface toxicity than to lack of efficacy. The preservative, benzalkonium chloride (BAK), is a key culprit.
Dr. Mangan concurs that BAK-related ocular surface toxicity is a common problem accompanying the use of generic medications.
“I am a dry eye specialist, and I often see patients with glaucoma who are being treated with one or more generic IOP-lowering medications and have significant ocular surface disease,” he says.
“With branded medications, we have options that are preservative-free or formulated with a non-BAK preservative that is gentler to the ocular surface. I have also seen exacerbation of ocular surface disease after patients were switched from branded preservative-free tafluprost 0.0015% (Zioptan; Akorn) to a BAK-containing generic prostaglandin analogue.”
Dr. Mangan says that the sequelae of ocular surface toxicity in these patients include adverse effects on comfort and vision. Furthermore, patients with conjunctival inflammation from topical antiglaucoma medication use are also at risk for trabeculectomy failure should surgery become indicated.
“Although a generic medication containing BAK can be acceptable for short-term use, there can be significant clinical ramifications from long-term exposure to this preservative,” he says.
Dr. Mangan says that his personal experience with generic medication-related problems also includes patients who had wound healing problems and worsening of dry eye disease when they received a generic nonsteroidal anti-inflammatory drug (NSAID) dosed four times a day instead of the once-daily NSAID that he prescribed. In addition, he has patients who developed rebound iritis after switching from branded prednisolone acetate 1% suspension (Pred Forte, Allergan) to a generic version.
He also cites the case of a patient being treated for herpes simplex keratitis whose condition improved after initiating treatment using a sample of a branded antiviral medication (ganciclovir ophthalmic gel, 0.15%; Zirgan, Bausch + Lomb), but subsequently worsened when she continued therapy with generic trifluridine.
“Ultimately, the patient did well but only after being seen at multiple extra visits that probably would not have been needed had she stayed on the branded medication,” Dr. Mangan says.
Such cases draw attention to the fact that there are branded medications without a generic alternative that offer clinical advantages because of their active ingredients, recommended dosing frequency, or ocular surface safety.
For example, Dr. Bowling says that when treating vision-threatening bacterial keratitis or severe conjunctival infection, besifloxacin ophthalmic suspension 0.5% (Besivance, Bausch + Lomb) is his antibiotic of choice because it has the highest in vitro activity against common Gram-positive causative pathogens among all fluoroquinolones.22
For controlling significant corneal or anterior segment inflammation, he likes to prescribe difluprednate ophthalmic emulsion 0.05% (Durezol, Alcon) that stands out for its potency and nonsettling formulation that in contrast to a suspension, obviates the need for shaking.
For patients with dry eye disease, Dr. Bowling uses lifitegrast ophthalmic solution 5% (Xiidra, Shire) that has a different mechanism of action and an indication for treating both signs and symptoms of dry eye disease.
“I want the ‘heavy hitter’ options I have with branded medications when I have patients with significant inflammation or infection that can lead to permanent tissue damage,” he says.
Cost considerations
Economics can drive the decision to prescribe a generic alternative. Nevertheless, choosing a generic medication does not necessarily translate into substantial cost savings. Rising costs of some generic ophthalmic medications is one factor that is leveling the cost difference.
A study analyzing data from five national pharmacy chains found that from 2014 to 2015, costs for generic latanoprost, timolol, dorzolamide, timolol/dorzolamide, brimonidine 0.15%, and brimonidine 0.2% increased significantly more than the national inflation rate, changing by as much as 45 percent.23 Significant increases in the cost of generic phenylephrine and prednisolone acetate have also been reported.2,24
“Optometrists are well aware of how the cost has risen for phenylephrine that we use in the office for dilation,” Dr. Bowling says. “I think that speaks to the fact that generic does not equate with inexpensive.”
Dr. Mangan says he is surprised at times by the lack of a significant cost difference between generic and branded medications.
“I used to think that the cost of a preservative-free glaucoma medication could be prohibitive for some patients, but it can be very competitive compared with a product containing a preservative, depending on the person’s insurance,” he says.
If cost is a concern, the availability of samples can allow patient access to some branded medications when short-term treatment is needed. Samples provided by branded medication manufacturers also give doctors the opportunity to gain familiarity with new products, says Dr. Bowling.
Furthermore, cost-saving opportunities are usually available for branded medications. These include patient assistance programs, coupons, discounts, and rebates provided by most if not all manufacturers of branded drugs as well as through other organizations.
Dr. Bowling and Dr. Mangan mention these opportunities to patients, and further details and assistance are provided by other staff.
Practical decisions
Concerns about generic medications are more relevant under some circumstances than others. Dr. Mangan says he finds it acceptable to prescribe a generic product for patients with a mild condition that requires relatively short-term treatment. For example, he will prescribe a generic antibiotic for someone with mild conjunctivitis.
However, he believes branded medications have value for use in postsurgical regimens, patients with a potentially sight-threatening and/or chronic condition, and for anyone with an already compromised cornea.
Similarly, Dr. Bowling says he might offer a generic medication for a condition in which vision is not at stake, such as a mild conjunctival infection or seasonal allergic conjunctivitis when the patient is happy with the control provided by a generic.
“Generic medications have a place, and I use them in my practice,” he says. “But for patients with a condition that is serious or that can quickly deteriorate, such as for a severe corneal infection or corneal ulcer, uveitis, corneal stromal inflammation, highly elevated or difficult to control IOP, as well as for patients with dry eye disease, I insist on a branded medication because I have confidence in its efficacy and safety.”
However, cost can be a concern.
“Cost is a problem for many patients in my practice population, and saving money can appeal to anyone, regardless of economic status,” Dr. Bowling says. “But cost shouldn’t decide what is right for the patient.”
Counseling conversations
Research shows that patients may not be forthcoming with their doctors if they have concerns about the cost of their medication.25 Therefore, it is important that clinicians ask questions to identify if cost presents a concern. Because many patients assume that the only difference between a branded and generic medication is cost, education is key.
Dr. Mangan says he tells patients the reasons why he is prescribing a branded product.
“I outline why I believe the branded medication is best given their conditions,” he says. “I explain that because of less stringent requirements for the approval of generic medications, there can be variability in the product and therefore in its efficacy, safety, and tolerability. In addition, I explain that generic medications may contain preservatives or inactive ingredients that can exacerbate or worsen ocular surface disease and even lead to decreased vision.”
He also mentions the cost factor.
“I address the financial aspect by explaining that the cost of generics has increased over the last few years,” he says. “In addition, I say that considering the tangible and intangible costs that can be incurred with a generic medication, the monetary savings may not be as significant as they think.”
Dr. Mangan says that when patients understand all of the relevant challenges and weigh both the direct and indirect costs associated with generic medications, even those who requested a generic medication often recognize that it makes more sense to strongly consider the branded product.
“Ultimately, it is the patient’s decision, and some patients will still choose to go the generic route. But I can sleep at night knowing that I provided appropriate counseling so that they could make an informed decision,” he says.
Dr. Bowling says his thoughts and practices always center around what he believes is best for each patient.
“I tell patients when I think a generic medication is appropriate or if I think the branded medication is best, and in the latter situation, I emphasize that they should be sure to get the prescription filled exactly as it is written,” he says.
Pharmacy substitutions
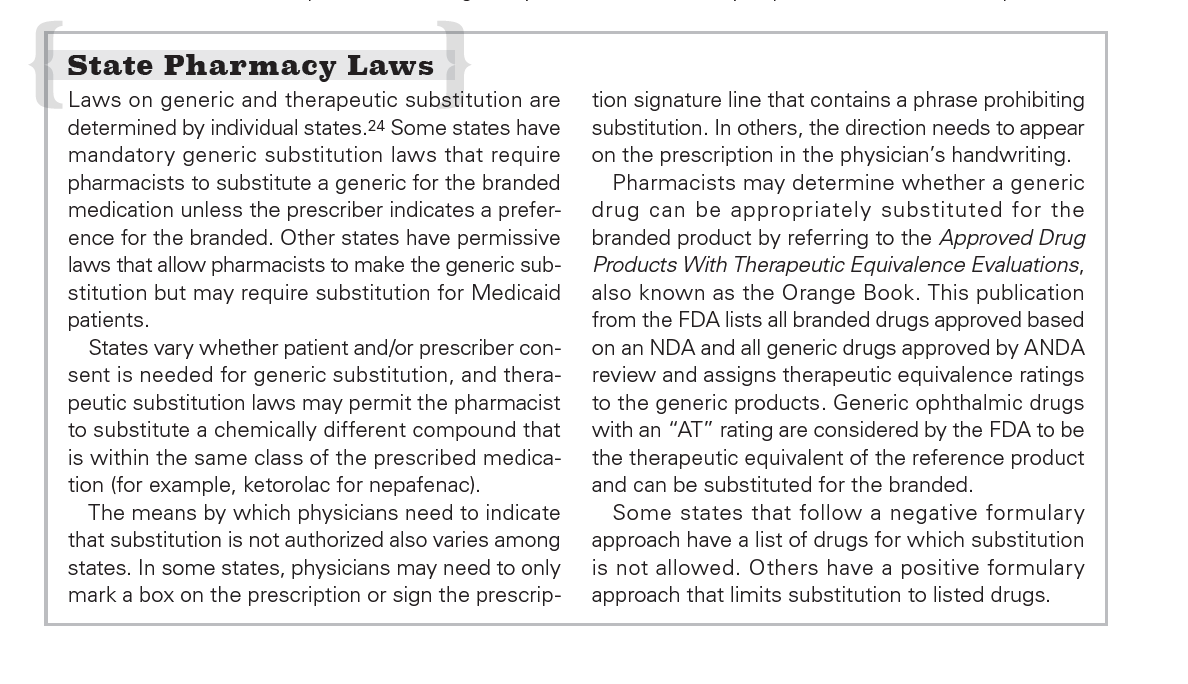
Awareness of state pharmacy laws pertaining to generic and therapeutic substitution is important for limiting a switch from a branded to a generic product when patients fill their prescriptions, and these laws vary widely from state to state [see sidebar: State Pharmacy Laws].26
But the appropriate notation on the prescription order does not guarantee against substitution, says Dr. Mangan.
“I have seen patients have a prescription for a branded product filled with a generic,” he says. “Taking the time to educate patients so that they will insist on the branded product is the most important step we can take in assuring the prescription gets filled as written.”
Dr. Bowling says that calls from pharmacists asking for permission to substitute a medication are not infrequent. In Georgia, pharmacists are permitted to make a generic substitution unless “Brand Necessary” was written on the prescription.
“It is disconcerting that the clinical decision I made after examining the patient can be usurped by someone who lacks my expertise and knowledge of the situation,” he says. “It puts the patient and my license at risk if something goes wrong.”


Maintaining vigilance
Partly because of the potential for substitutions being made without their consent, Dr. Bowling and Dr. Mangan instruct all patients to bring their medications with them to their follow-up visits. For situations in which patients choose a generic against their recommendations, they plan for closer follow-up.
“If a patient has glaucoma comorbid with dry eye disease and is using a generic medication for IOP control, I expect the generic will worsen the dry eye disease and ask the patient to return sooner than normal for the next follow-up visit,” Dr. Mangan says. “When treating a corneal infection, I will also see patients sooner and more frequently if they have disregarded my recommendation of a branded antimicrobial agent.”
Concluding comments
Authors of the study describing eyecare providers prescribing of generic and brand name medications based on analyses of Medicare Part D data suggested that inducements from manufacturers of brand name products were a potential factor limiting greater use of generics.2 The idea is ludicrous, says Dr. Mangan.
“Eyecare professionals will use a generic drug when they believe it can match the efficacy, safety, and tolerability of a branded medication and also provide a significant cost savings to the patient. Otherwise, the reliability of a branded product makes it the better choice.”
As a bottom line, however, patients can ultimately make the decision of whether they are treated with a branded or generic medication, and that underscores the importance of patient education.
“Sometimes if you are behind schedule, five room lights are blinking, and your technician is kicking your chair to get you moving, the easiest thing to do is to prescribe a generic medication,” Dr. Mangan says. “I think it is very important to consider the potential benefits of a branded medication and the trade-offs that can accompany generics and take the time to explain the facts to patients.”
“Furthermore, we cannot always assume that the generic medication will be cheaper and more cost effective than the branded product or that coverage for a newer branded medication will be less favorable than for an older branded product,” he says. “Sometimes patients are on a fixed income and simply cannot opt for the branded product, but the margin of separation can be less than expected. When patients understand the concerns, they can be more than willing to pay the extra money to get the reliable branded product with its reproducible quality and proven efficacy and safety.”
Dr. Bowling also disputes the idea that doctors’ prescribing behavior is influenced by industry. In addition, he emphasizes the importance of educating patients about reasons for favoring a branded medication and says that he finds he is spending an increasing amount of time on calls from pharmacists seeking permission to substitute a generic and on paperwork and phone calls obtaining prior authorization from insurers for use of branded medications.
“If I believe it is important enough to prescribe a branded product because it is best for the patient, then I feel it is my responsibility to spend time counseling patients about the reasons, explaining the need to the pharmacist, and advocating for patients to insurance representatives,” Dr. Bowling says.
Dr. Bowling also reminds colleagues that generics exist only because there was a branded medication to copy.
“Prescribing only generics ignores the continuing importance of newer medications to our patients’ health. If only generics were available, drug developers would have little opportunity to develop new products,” he says.
References:
1. Association for Accessible Medicine. Generic Drug Access & Savings in the U.S. 2017.
http://accessiblemeds.org/sites/default/files/2017-07/2017-AAM-Access-Savings-Report-2017-web2.pdf. Accessed 10/8/18.
2. Newman-Casey PA, Woodward MA, Niziol LM, et al. Brand medications and Medicare Part D: how eye care providers’ prescribing patterns influence costs. Ophthalmology. 2018;125(3):332-339.
3. U.S. Food and Drug Administration. Abbreviated New Drug Application (ANDA). https://www.fda.gov/drugs/developmentapprovalprocess/howdrugsaredevelopedandapproved/approvalapplications/abbreviatednewdrugapplicationandagenerics/default.htm. Accessed 10/8/18.
4. U.S. Food and Drug Administration. CFR - Code of Federal Regulations Title 21. http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=314.94. Accessed 10/8/18.
5. U.S. Food and Drug Administration. Current good manufacturing practice (CGMP) regulations. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/Manufacturing/ucm090016.htm. Accessed 10/8/18.
6. Chambers WA. Ophthalmic generics–are they really the same? Ophthalmology. 2012;119(6):1095-1096.
7. Choi SH, Lionberger RA. Clinical, pharmacokinetic, and in vitro studies to support bioequivalence of ophthalmic drug products. AAPS J. 2016;18(4):1032-1038.
8. U.S. Food and Drug Administration. Draft Guidance on Cyclosporine. https://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/ucm358114.pdf. Accessed 10/8/18.
9. U.S. Food and Drug Administration. Draft Guidance on Difluprednate. https://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm481813.pdf. Accessed 10/8/18.
10. U.S. Food and Drug Administration. ANDA Submissions-Amendments to Abbreviated New Drug Applications Under GDUFA Guidance for Industry. https://www.fda.gov/downloads/Drugs/Guidances/UCM404440.pdf. Accessed 10/9/18.
11. Angmo D, Wadhwani M, Velpandian T, et al. Evaluation of physical properties and dose equivalency of generic versus branded latanoprost formulations. Int Ophthalmol. 2017;37(2):423-428.
12. Kahook MY, Fechtner RD, Katz LJ, et al. A comparison of active ingredients and preservatives between branded and generic topical glaucoma medications using liquid chromatography-tandem mass spectrometry. Curr Eye Res. 2012;37(2):101-108.
13. Kolko M, Koch Jensen P. The physical properties of generic latanoprost ophthalmic solutions are not identical. Acta Ophthalmol. 2017;95(4):370-373.
14. Mammo ZN, Flanagan JG, James DF, Trope GE. Generic versus brand-name North American topical glaucoma drops. Can J Ophthalmol. 2012;47(1):55-61
15. Marando CM, Seibold LK, SooHoo JR, et al. The utility of cap color and bottle characteristics for topical glaucoma therapy. Ophthalmology. 2015;122(12):2577-2578.
16. Kim DH, Addis VM, Pan W, VanderBeek BL. Comparative effectiveness of generic latanoprost versus branded prostaglandin analogs for primary open angle glaucoma. Ophthalmic Epidemiol. 2018 Sep 6:1-9.
17. Diagourtas A, Kagelaris K, Oikonomakis K, et al. Prospective study comparing Xalatan eye drops and two similar generics as to the efficacy and safety profile. Eur J Ophthalmol. 2018;28(4):378-384.
18. Egan P, Harris A, Siesky B, et al. Comparison of intraocular pressure in glaucoma subjects treated with Xalatan® versus generic latanoprost. Acta Ophthalmol. 2014;92(5):e415–e416.
19. Stewart WC, Sharpe ED, Stewart JA, Hott CE. The safety and efficacy of timolol 0.5% in xanthan gum versus timolol gel forming solution 0.5%. Curr Eye Res. 2002;24(5):387-391.
20. European Glaucoma Society. Treatment principles and options. In: Terminology and Guidelines for Glaucoma, 4th ed. Savona, Italy: PubliComm; 2014:130-195.
21. Flach AJ. Corneal melts associated with topically applied nonsteroidal anti-inflammatory drugs.Trans Am Ophthalmol Soc. 2001;99:205-210; discussion 210-212.
22. Asbell PA, Mah FS, Sanfilippo CM, DeCory HH. Antibiotic susceptibility of bacterial pathogens isolated from the aqueous and vitreous humor in the Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR) surveillance study. J Cataract Refract Surg. 2016;42(12):1841-1843.
23. Yook E, Fechtner RD, Khouri AS. Generic glaucoma medication costs: a 2 year analysis [Abstract 5585]. Poster presented at ARVO 2016. Seattle, WA, May 4, 2016.
24. Schondelmeyer SW, Purvis L. Rx Price Watch Report. Trends in Retail Prices of Generic Prescription Drugs Widely Used by Older Americans, 2006 to 2015.
https://www.aarp.org/content/dam/aarp/ppi/2015/trends-in-retail-prices-of-generic-prescription-drugs-widely-used-by-older-americans.pdfh B. Accessed 10/8/18.
25. Slota C, Davis SA, Blalock SJ, et al. Patient-physician communication on medication cost during glaucoma visits. Optom Vis Sci. 2017;94(12):1095-1101.
26. Generic drug substitution requires pharmacist attention to ensure compliance with state laws and regulations. Newsletter. National Association of Boards of Pharmacy. 2013;42(6):135, 136, 140.
Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.
















