
EDOF contact lens focuses on pediatric myopia control
Clinical pilot study evaluates effect after 1 month of wear.
Across the globe, an estimated 23% of the world’s population has been diagnosed with myopia—and of that, 2.7% of those people have high myopia.1
By 2050, an estimated 50% of the global population will be diagnosed with myopia.1



Our research group recently conducted a pseudo-experimental, prospective, longitudinal clinical pilot study at the Optometric Clinic of the University of Alicante, Spain, to evaluate the impact during the first month of wear of a new extended depth-of-focus (EDOF) contact lens for myopia control:
Mylo (Mark’ennovy).2
This lens is composed of silicone hydrogel and is designed for monthly replacement. The material has a high water content (75%) and a low coefficient of friction (0.02).
The intraocular lens (IOL) can be manufactured with a great variety of radii of curvature (7.10 to 9.80 mm), diameters (13.50 to 15.50 mm), and negative optical powers (0.25 to 15.00 D) to customize the fit.
From the optical perspective, this lens is based on a distribution of power from the center to the periphery—which is not
progressive—especially in the optical zone, which includes nonmonotonic and aperiodic variation of powers (Figure).2,3

")
Figure: Power profile of the Mylo, a new extended depth-of-focus contact lens. (Image courtesy of Mark’ennovy)
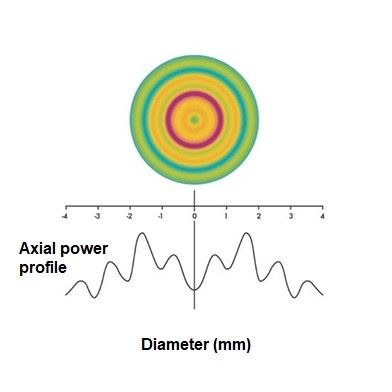
This complex optical surface leads to controlled induction of high-order aberrations, especially primary (Z40) and secondary (Z60) spherical aberrations, allowing an enlarged depth of focus and, consequently, the relative maintenance of its optical behavior under different circumstances (pupil aperture, centration, and corneal optical properties).
Proprietary nonlinear optimization algorithms for high-order aberrations are used to generate these complex surfaces.3,4
Contact lens trial
We recruited a total of 30 eyes from 15 subjects with an average age of 13.3 ± 0.7 years.
Mean monocular and binocular best spectacle-corrected prefitting visual acuities were –0.02 ± 0.04 and –0.04 ± 0.06 logMAR, respectively, when measured at far.
For near, corresponding values were –0.02 ± 0.05 and –0.06 ± 0.05 logMAR, respectively.There was a statistically significant reduction in visual acuity when comparing these spectacle-corrected values with those obtained from the first test with the newly fitted contact lens (P ≤ .004).
However, there were no significant differences in monocular and binocular distance and near visual acuities when comparing values measured with spectacles before lens fitting vs those measured with the lens at the end of the follow-up (P ≥ .34).
There was a mean reduction of the accommodative lag of 0.30 D (P < .001) without associated alterations in the magnitude of phoria and fusional vergence (P ≥ .066). With the contact lens, a controlled but statistically significant increase (P ≤ .005) was found in ocular high-order aberration root mean square (RMS), primary coma RMS, primary spherical aberration Zernike term, and secondary astigmatism RMS.


Most subjects described the perception of photic phenomena as being no bother both before and at the end of the follow-up (glare, 93.3% vs 76.9%, P = .569; halos, 93.3% vs 84.6%, P = .657; starbursts, 53.3% vs 53.8%, P = .162). No significant variations were found in terms of mean keratometry (P = .329) or axial length (24.50 ± 0.17 mm vs 24.54 ± 0.20 mm, P = .285), indicating the absence of molding or modification of the corneal geometry after the use of the lens and progression of myopia during the study period.
However, a statistically significant
reduction was found in anterior chamber depth, from a mean value of 3.40 ± 0.03 mm at the prefitting visit to 3.34 ± 0.04 mm after 30 days of contact lens use (P = .022).
No severe ocular complications were reported during the period of lens use. In the fitting process, 3 subjects (20%) required changes in the parameters of the first lens tested due to centration and movement problems (change of base curve).
Conclusion
The evaluation of the EDOF contact lens indicated it provides adequate visual acuity and quality, with associated increases of several high-order aberrations and a trend toward reduction of accommodative lag that should be confirmed in future studies.
Other changes found in the current series, such as the reductions in pupil size measured under photopic conditions and in anterior chamber depth, should be investigated further to confirm their real relationship with the effect of the lens.
More research, an increase in sample size, and the inclusion of a control group are needed to investigate how all these changes are related as well as how they control eyeball elongation.
References
1. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-1042. doi:10.1016/j.ophtha.2016.01.006
2. Corpus G, Piñero DP. Short-term effect of wearing of extended depth-of-focus contact lenses in myopic children: a pilot study. Appl Sci. 2022;12(1):431. doi:10.3390/app12010431
3. Bakaraju RC, Ehrmann K, Ho A. Extended depth of focus contact lenses vs. two commercial multifocals: part 1. Optical performance evaluation via computed through-focus retinal image quality metrics. J Optom. 2018;11(1):10-20. doi:10.1016/j.optom.2017.04.003
4. Bakaraju RC, Tilia D, Sha J, et al. Extended depth of focus contact lenses vs. two commercial multifocals: part 2. Visual performance after 1 week of lens wear. J Optom. 2018;11(1):21-32. doi:10.1016/j.optom.2017.04.001
Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.










 of patients believe that medical technology innovations will enhance care for the aging population, with 90% of providers recognizing the need to address specific requirements for older patients. Image credit: AdobeStock/buritora")






