
Minimally invasive surgical solutions for presbyopia
Presbyopia, an age-related loss of accommodative amplitude of the eye resulting in near and intermediate vision deficits, begins to affect most people once they reach their early 40s.
Presbyopia, an age-related loss of accommodative amplitude of the eye resulting in near and intermediate vision deficits, begins to affect most people once they reach their early 40s. Although easily managed with corrective glasses, some natural emmetropes-particularly individuals who became emmetropic after undergoing laser vision correction-prefer to remain spectacle-free.
Contact lens monovision that targets the non-dominant eye for near vision is a longstanding and widely used approach for treating emmetropic presbyopia.
Related: Managing presbyopia with surgery
However, this option is not ideal for everyone. Not all individuals adapt to contact lens monovision. Some patients do not consider contact lens wear an acceptable alternative to spectacles. Even individuals who are successful with contact lens monovision must accept compromises that include decreased distance vision in the non-dominant eye and reduced stereopsis.
The search for surgical solutions for presbyopia has led to the development of pseudophakic intraocular lenses (IOLs) that use various optic designs to provide an extended range of uncorrected functional vision. Most individuals ages 40 to 60 years old, however, have a clear crystalline lens and do not need cataract surgery.
For these patients, corneal inlays offer a minimally invasive surgical approach for treating presbyopia.
Presbyopia-correcting inlays
Treatment of presbyopia with a corneal inlay is a monocular procedure that involves placement of the device into the non-dominant eye.
Two devices, Kamra inlay (AcuFocus) and Raindrop Near Vision Inlay (ReVision Optics), are approved by the U.S. Food and Drug Administration (FDA) with indications for use in phakic presbyopes who have minimal spherical refractive error and do not require glasses or contact lenses for clear distance vision (see Table 1).
Related: New correction option for presbyopes
A third corneal inlay, Flexivue Microlens (Presbia), is under investigation in a premarketing clinical trial.
Outside of the United States, corneal inlays are being used in pseudophakic presbyopes and in combination with laser vision correction surgery. Raindrop Near Vision Inlay is being evaluated in an ongoing clinical trial for presbyopia correction in emmetropic pseudophakic patients.
The three inlays have different designs and correct presbyopia via different mechanisms.
Results from FDA studies for both the Kamra inlay and Raindrop Near Vision Inlay showed patients achieved very good near and intermediate uncorrected visual acuity.1 Maintenance of good uncorrected binocular distance vision is a feature of all of the corneal inlays.2
Related: Looking into the future of presbyopia treatments
Visual recovery after corneal inlay surgery can take as long as four to six weeks, but the minimally invasive surgery has a very good safety profile.
In the FDA study, there was rare removal for cosmesis or an immunologic response that can result in fibrosis necessitating inlay removal.1 Inlay removal is easily accomplished for a complication or because the patient is dissatisfied with the outcome.
Once the inlay is removed, patients should return to a refractive result that is close to their preop vision within four to six weeks.
Kamra inlay


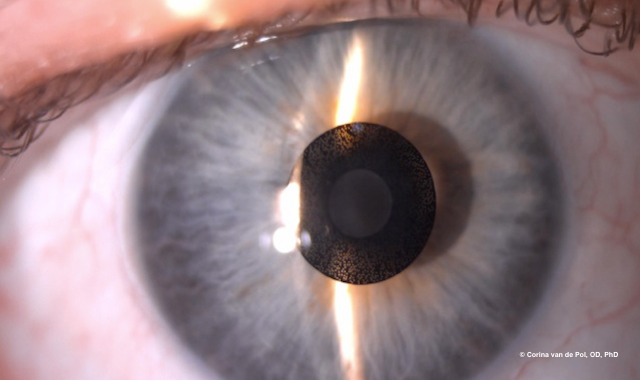
Figure 1 - Kamra inlay 8.5 years post implantation.
Kamra inlay is the first corneal inlay that was approved by the FDA for treatment of presbyopia. Made of polyvinylidene fluoride (PVDF), Kamra is an annulus with an opaque outer ring and central opening. Analogous to the f-stop of a camera, its small aperture acts via a pinhole effect to increase depth of field.
The design of Kamra has evolved over time. The current version is a third-generation iteration that measures 5 µm in thickness and 3.8 mm in total diameter and features a 1.6 mm central aperture.
The PVDF ring contains a total of 8,400 microperforations, each 5 to 11 µm in diameter, that enable nutrient flow and are placed in a pseudorandom pattern that minimizes the potential for causing unwanted visual symptoms.
Related: Preventing lens dropout with presbyopic patients
Originally Kamra inlay was placed under a LASIK-like flap, but it is now inserted into a pocket deep into the cornea. This approach minimizes any immunologic responses and subsequent fibrotic reaction, the company learned through trial and error. The pocket is created using a femtosecond laser, and the procedure also requires a special instrument that is attached to the surgical microscope to guide centration (AcuTarget HD, AcuFocus).
The Kamra inlay has been safe, well-tolerated, and associated with good patient satisfaction.1
Because it creates an artificially small pupil, however, contrast sensitivity in the implanted eye is reduced under mesopic conditions.1 For that reason, the Kamra inlay may not be a good option for individuals who spend a significant amount of time driving at night.
In addition, some people with light colored irides may object to the cosmetic appearance of the dark PVDF ring.1
Related: Letters to the editor: Presbyopia patients, online appointing
Raindrop Near Vision Inlay

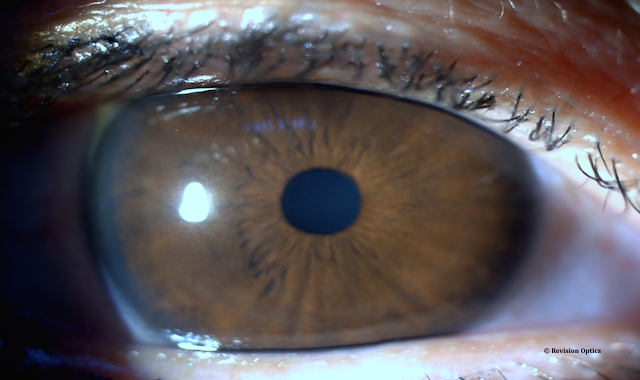
Figure 2 - Raindrop Near Vision Inlay in the eye.
The Raindrop Near Vision Inlay is a clear meniscus-shaped lens that is 2.0 mm in diameter and 32 µm thick in the center. It is made of a high-water content hydrogel material that is biocompatible and highly permeable.
The inlay is implanted under a flap, which is created using a femtosecond laser at approximately one-third corneal thickness, and then centered over a light-constricted pupil.
Aside from a femtosecond laser, no other special equipment is needed to place the Raindrop.


Figure 3 - Retroillumination of Raindrop inlay.
Its mechanism of action involves corneal reshaping. Raindrop creates a gentle profocal cornea with a smooth transition from near to distance vision.
Related: Presbyopia to impact more than 2 billion people worldwide by 2020, Alcon forecasts
Contrast sensitivity may be slightly reduced by Raindrop Near Vision Inlay, but the potential for this effect is less than with the Kamra inlay.2
Flexivue Microlens


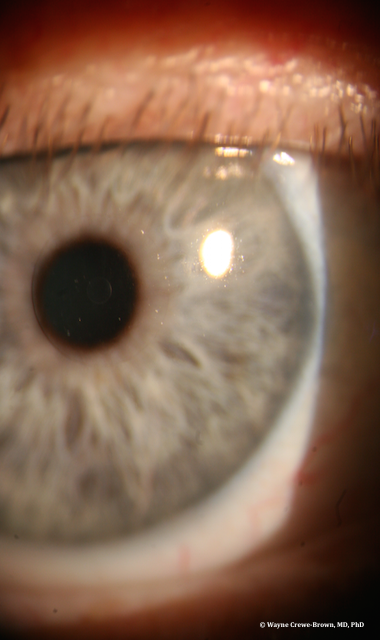
Figure 4 - Slit lamp view of Presbia Flexivue Microlens in place.
Flexivue Microlens is an add power inlay that is currently being investigated in a U.S. FDA trial.
It is made of hydroxyethyl methacrylate and methyl methacrylate with an ultraviolet blocker. The hydrophilic acrylic material is clear, biocompatible, permeable, and has a higher refractive index than the cornea.
Flexivue Microlens measures 3.2 mm in diameter and 15 µm thick at the edge; central thickness depends on the add power of the inlay. It has an annular design with a small central hole that facilitates nutrient flow, a surrounding plano zone, and an outer optic zone of varying powers in the range from +1.50 D to +3.50 D.
Flexivue Microlens inlay is placed into a femtosecond laser-created corneal pocket.
Related: The pros and cons of clear lens exchange
Scleral surgery

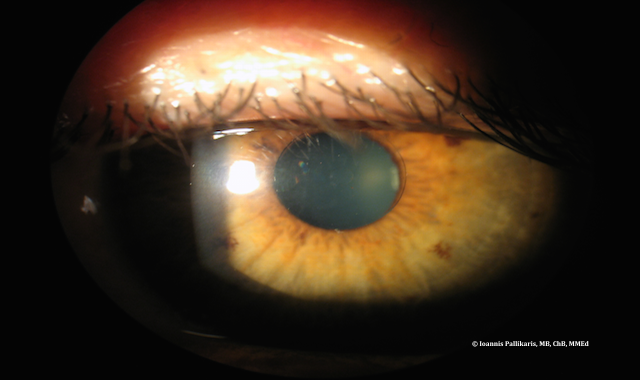
Figure 5 - Slit lamp view of Presbia Flexivue Microns in place.
Scleral implant surgery with VisAbility implant system (Refocus) is another approach for presbyopia correction that is under investigation in an ongoing clinical trial in the United States.
In this procedure, four polymethylmethacrylate plastic segments are placed into scleral tunnels in order to expand the scleral tissue around the crystalline lens and enable accommodation. A four-to-six-week recovery period is also needed before patients develop good near vision, the FDA study group learned.
The surgical procedure has evolved over time and new instrumentation makes segment implantation easier and more precise, according to investigators.
The scleral procedure can provide a full range of vision. In fact, it can result in better near vision than the inlay procedures because it is a binocular approach.
Other advantages compared with corneal inlay procedures are avoidance of the visual axis and the potential for corneal immunologic reactions that can interfere with vision. The surgery, however, is more invasive, and its benefit is lost if cataract surgery is needed and the crystalline lens is removed.
Related: 3 correction options for presbyopes
Presbyopia and surgery
The development of safe and effective surgical methods for correcting presbyopia has been the Holy Grail in ophthalmology.
Although there is yet no perfect solution, the availability of an expanding armamentarium of options makes this a very exciting time for refractive surgeons and their staff and patients who desire reduced spectacle-dependence.
References
1. AcuFocus. Kamra Inlay Professional Use Information. Available at:http://www.accessdata.fda.gov/cdrh_docs/pdf12/P120023d.pdf. Accessed 11/28/16.
2. Whitman J, Dougherty PJ, Parkhurst GD, Olkowski J, Slade SG, Hovanesian J, Chu R, Dishler J, Tran DB, Lehmann R, Carter H, Steinert RF, Koch DD. Treatment of presbyopia in emmetropes using a shape-changing corneal inlay: one-year clinical outcomes.Ophthalmology. 2016 Mar;123(3):466-75.
Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.







