Know the basics of a pediatric eye exam
Binocular testing, extraocular movements, dilation, and visual acuity are reviewed




Some ODs feel nervous when they see a pediatric patient on their schedule. For several reasons, the examination sequence for a pediatric eye exam is different from an adult eye exam. First, the attention span of a child is limited. ODs must be quick and selective in their exam sequence to obtain quality information. Second, all new pediatric patients must be sufficiently dilated and cyclopleged. Unlike adult patients who can be refracted behind a phoropter, most children will need their refractive error neutralized by retinoscopy. The most accurate way to perform retinoscopy on a child is with relaxed accommodation. Finally, the most important items to evaluate in the pediatric population are the presence of amblyopia or strabismus and ocular health.
Let’s review the pediatric exam sequence.
Binocular testing
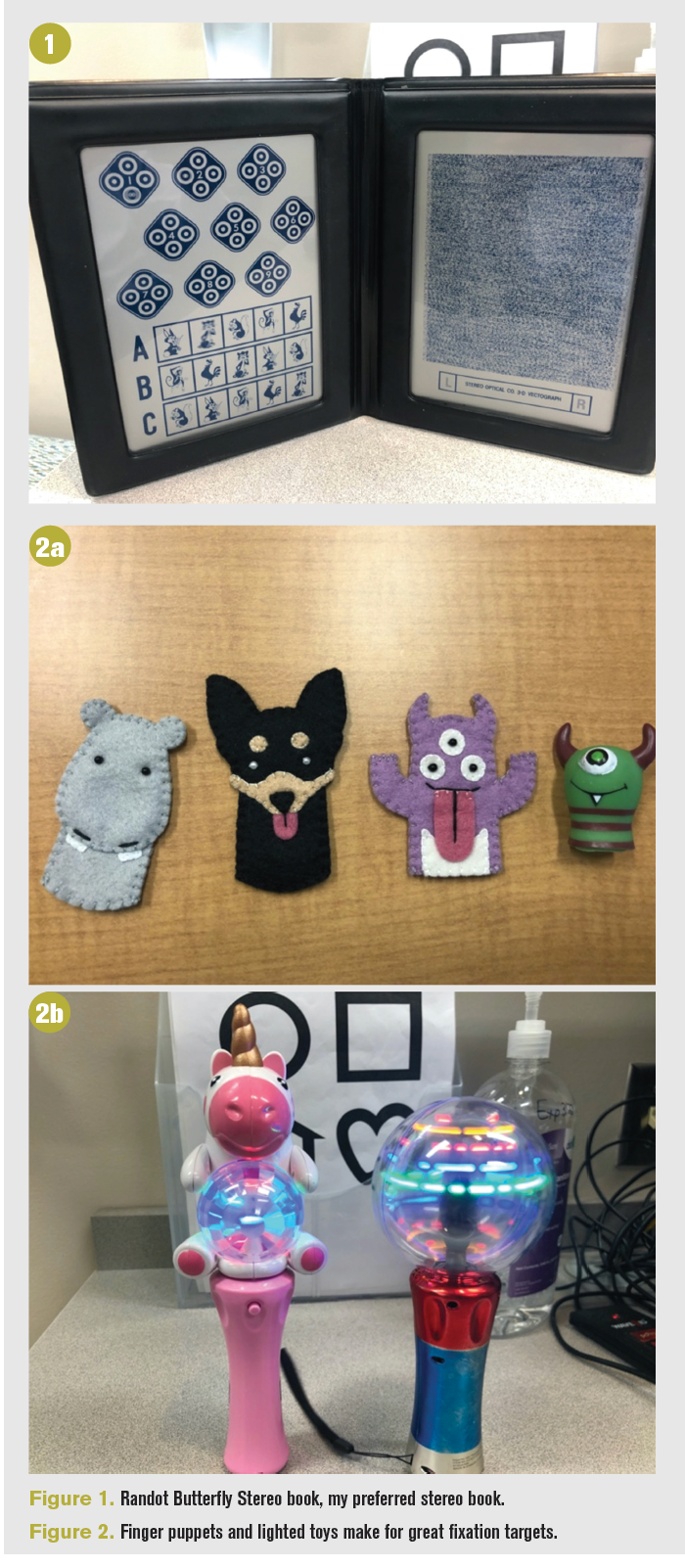
In a pediatric eye exam, I recommend performing binocular testing first before monocular testing. The binocular tests allow ODs to evaluate the child’s binocular status when the child is most alert. The longer the duration of the exam, the more the child will fatigue and some monocular tests will cause the patient’s eyes to dissociate. Therefore, the first test in my pediatric exam sequence is the Randot Stereo test (Figure 1). If a child can correctly identify the butterfly in this book, I know the child has acceptable stereopsis and binocularity.
The binocular test result is a helpful piece of information that builds the child’s clinical picture. Proceeding through the exam sequence, the more information ODs obtain from pediatric patients, the more of a clinical picture ODs can build. However, situations and times exist when the child is uncooperative, shy, or unable to participate because of medical conditions. Thus, gaining stereo information is helpful but not crucial in the assessment and treatment of pediatric patients.
Various stereo books are available. I personally do not find the stereo fly to be helpful in determining stereopsis because it is difficult to ask a 3-year-old to touch or pinch the wings of the fly. Compared to the butterfly, it is more difficult to be certain that your pediatric patient has stereopsis based on the fly.
After stereopsis testing, the OD can transition to the Worth 4 Dot test. The child switches from wearing the stereo glasses to the red-green glasses. Ask how many circles the child sees. How many green circles? How many red circles? Remember that the red filter covers the right eye and the green filter covers the left eye. This test is a fun and easy way to subjectively determine suppression based on the patient’s response. If the child reports seeing 2 red circles, then the child is suppressing their left eye. Conversely, if the child reports seeing 3 green circles, then the child is suppressing their right eye.
Extraocular movements
Next in the exam sequence is testing extraocular movements. Finger puppets or lighted toys (Figure 2) are exciting fixation targets for the pediatric patient. Alternatively, a doll’s eye maneuver can determine a pediatric patient’s extraocular movements. I play a movie at the other end of the room, and I ask the patient to watch the movie as I move their head to determine the range of motion The anatomy of the extraocular muscles with the insertion points on the eye help determine the eye’s movement. The medial and lateral rectus adduct and abduct the eye. The superior and inferior rectus muscles (vertical recti) insert onto the eye at a 23˚ angle from midline. The superior rectus elevates, intorts, and adducts, and the inferior rectus depresses, extorts, and adducts. Conversely, the oblique muscles insert in an anterior to posterior fashion at 51˚ from midline. Thus, the superior oblique in primary gaze intorts, depresses, and abducts, and the inferior oblique extorts, elevates, and abducts.1
The extraocular muscles move the eyes in all directions. Test the eye muscles in the H formation. Evaluate each muscle to see for overaction, underaction, or misinnervation. When the patient looks to the right, the left eye’s superior oblique muscle is sufficiently isolated because the left eye positions perpendicular to the superior rectus muscle. This allows ODs to see a potential inferior oblique overaction or a superior oblique palsy.
During extraocular muscle testing, observe the patient for nystagmus or anomalous head posture. Characteristically, it has been thought that patients with a congenital superior oblique palsy will display a facial asymmetry or hemifacial microsomia because of a long-standing head tilt. However, the reliability of the facial asymmetry as being pathognomonic for superior oblique palsy should be used with caution. Results from one study illustrate that the anomalous head posture could arise from superior oblique palsy or a pulley heterotopy.2
With nystagmus, observe the patient to determine the presence or absence of nystagmus. If present, assess the type, frequency, and amplitude. The movie at the end of the exam lane helps when assessing nystagmus and pupils. It keeps the patient distracted by fixating into the distance as the OD assesses the eyes.
Different methods are used to perform a cover test: alternate, unilateral, Hirschberg, and Krimsky. For patients who are monocular, have poor visual acuity or are poor fixators, performing Hirschberg or Krimsky to determine ocular alignment may be sufficient. For older patients who are more attentive, perform a unilateral or alternate cover test.
Pediatric eye exam: Keys to success
Visual acuity
In addition, different methods are used to test visual acuity. Starting with the infants and toddlers, obtain visual acuity with Teller Acuity Cards. I set up the testing as a peek-a-boo game with patients as I flash the card in front of the infant and observe their eyes to see which side of the card they gravitate toward.
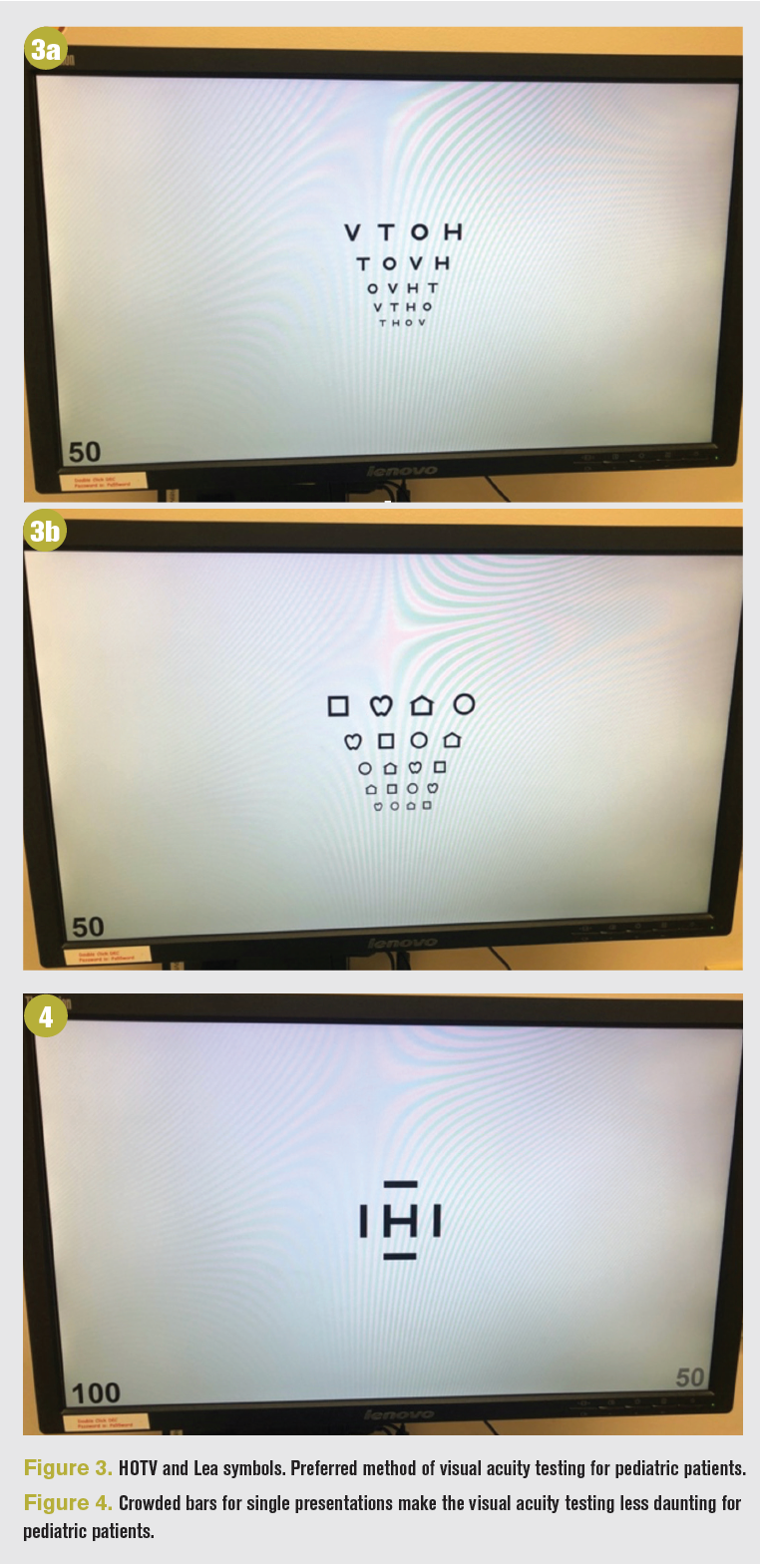
Preschool-aged children can perform matching games to determine their visual acuity. I use Lea symbols for younger patients and HOTV letters for older ones (Figure 3). I perform visual acuity testing as single letters with crowded bars (Figure 4). The crowded bars simulate a line of letters for the child, but the single-letter presentation makes the task seem not as daunting.
For elementary-aged children and older, I use standard Snellen symbols.
Evaluate a f ixation preference between the eyes with the induced tropia test. Place a prism of 14 to 16 mm pupillary distance in front of the patient’s eyes. The prism induces diplopia. If the patient has equal vision between the eyes, the patient will move their eyes between the 2 images. However, if the patient experiences worse visual acuity with the prism, no eye movement will be observed. Conversely, if the patient experiences better visual acuity with the prism, a single eye movement will be observed as the patient refixates on the new diplopic image. The induced tropia test reveals an approximately 2- to 3-line difference in visual acuity between the eyes.3
For patients unable to participate in the previously mentioned visual acuity testing, the central, steady, maintained (CSM) approach can help. The name relates to the patient’s fixation on a target. If each eye fixates centrally and not eccentrically, holds steady fixation on that target, and continues to stay fixated on that target even when occlusion is removed from the fellow eye, the vision is noted as “CSM.” Central and steady are monocular tests, and maintained is a binocular test.


Dilation
The dilated portion of the exam sequence is the most important part of the exam. There will be days or situations when the patient will not cooperate with exam components. The most essential parts of the evaluation are ensuring ocular health and determining refractive error. To obtain an accurate reading of a child’s refractive error, the OD must relax the patient’s accommodation. The 3 most common topical cycloplegic agents are atropine, cyclopentolate, and tropicamide.4 Because of the time to maximum cycloplegia and cycloplegic effect, cyclopentolate is the agent of choice for many ODs.
The most common cause for decreased vision in children, other than uncorrected refractive error, is amblyopia. Cycloplegic retinoscopy determines the extent of the patient’s refractive error. The American Academy of Ophthalmology and the American Optometric Association created amblyogenic refractive error guidelines.5,6
Prescribing glasses for pediatric patients is as much an art as a science. Ophthalmologists suggest that optometrists overprescribe glasses to children, causing a financial burden on the healthcare system.7 In prescribing for pediatric patients, the first step is knowing when to prescribe, and the second is knowing what to prescribe.
I determine glasses prescribing based on the answers to these questions:
– Does this refractive error have potential to cause amblyopia?
– How did the child perform on visual acuity testing?
– How did the child perform on stereoacuity testing?
– How old is the child? Is the child attending grade school?
– What is the parents’ socioeconomic background?
ODs and ophthalmologists differ in their prescribing patterns. Even among ODs, large variation exists. The following prescribing guidelines are my opinion. Every pediatric patient presenting for a comprehensive eye exam will have a refractive error with cycloplegic retinoscopy.8 My job is to determine the severity of the refractive error and whether this refractive error may cause amblyopia. I evaluate the level and magnitude of the refractive error and compare it to what is normal for a child this age.
For patients with myopia and astigmatism, I prescribe the full value of the refractive error, especially if the child is school aged. I often monitor low levels of myopia and astigmatism in toddlers and preschool children. For patients with hyperopia, I consider the level of error and its severity for the patient’s age. Unless the patient has esotropia, I prescribe a symmetrical reduction in hyperopia to both eyes, rarely giving their full cycloplegic refractive error.


References
1. Kanski J, Bowling B. Kanski’s Clinical Ophthalmology 8th Edition; 2015.
2. Velez FG, Clark RA, Demer JL. Facial asymmetry in superior oblique muscle palsy and pulley heterotopy. J AAPOS. 2000;4(4):233-239. doi:10.1067/mpa.2000.105277
3. Nanda KD, Blaha B, Churchfield WT, et al. Induced tropia test and visual acuity testing in nonverbal children. J Binocul Vis Ocul Motil. 2018;68(4):134-136. doi:10.1080/2576117X.2018.1525235
4. Egashira SM, Kish LL, Twelker JD. Comparison of cyclopentolate versus tropicamide cycloplegia in children. Optom Vis Sci. 1993;70(12):1019-1026. doi:10.1097/00006324-199312000-00005
5. Rouse MW, Cooper JS, Cotter SA, Press LJ, Tannen BM. Optometric clinical practice guideline care of the patient with amblyopia. American Optometric Association. Accessed May 20, 2021. https://www.aoa.org/AOA/Documents/Practice%20 Management/Clinical%20Guidelines/Consensus-based%20 guidelines/Care%20of%20Patient%20with%20Amblyopia.pdf
6. Wallace DK, Christianse SP, Sprunger DT, et al. Pediatric Eye Evaluations PPP – 2017. American Academy of Ophthalmology. November 2017. Accessed May 20, 2021. https://www.aao.org/ preferred-practice-pattern/pediatric-eye-evaluations-ppp-2017
7. Donahue SP. How often are spectacles prescribed to “normal” preschool children? J AAPOS. 2004;8(3):224-229. doi:10.1016/j. jaapos.2004.05.004
8. Lyons SA, Jones LA, Walline JJ, et al. A survey of clinical prescribing philosophies for hyperopia. Optom Vis Sci. 2004;81(4):233-237. doi:10.1097/00006324-200404000- 00008