
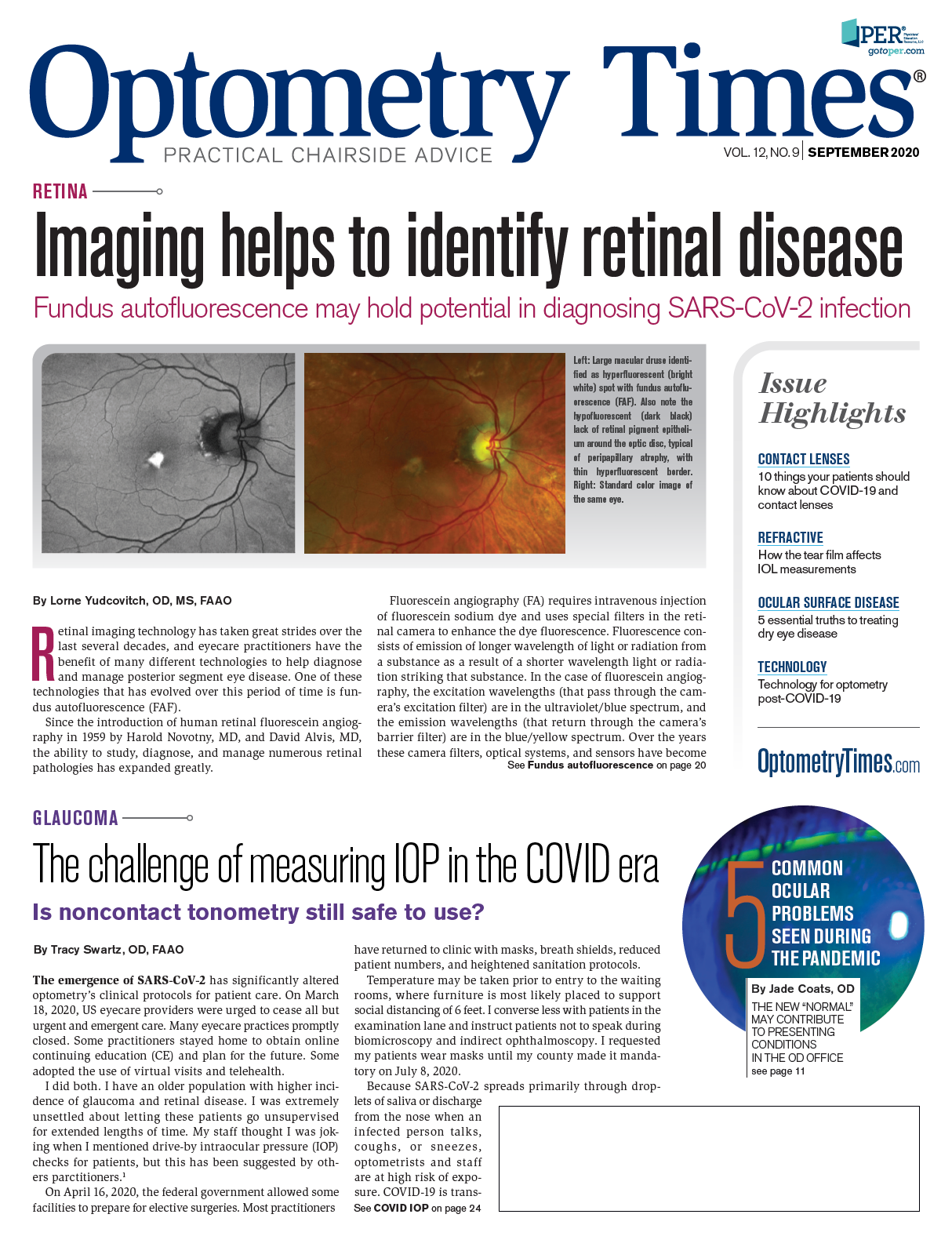
The challenge of measuring IOP in COVID era
Is noncontact tonometry still safe to use?



The emergence of SARS-CoV-2 has significantly altered optometry’s clinical protocols for patient care. On March 18, 2020, US eyecare providers were urged to cease all but urgent and emergent care. Many eyecare practices promptly closed. Some practitioners stayed home to obtain online continuing education (CE) and plan for the future. Some adopted the use of virtual visits and telehealth.
I did both. I have an older population with higher incidence of glaucoma and retinal disease. I was extremely unsettled about letting these patients go unsupervised for extended lengths of time. My staff thought I was joking when I mentioned drive-by intraocular pressure (IOP) checks for patients, but this has been suggested by others parctitioners.1
On April 16, 2020, the federal government allowed some facilities to prepare for elective surgeries. Most have returned to clinic with masks, breath shields, reduced patient numbers, and heightened sanitation protocols. Temperature may be taken prior to entry to the waiting rooms, where furniture is most likely placed to support social distancing of 6 feet. I converse less with patients in the examination lane and instruct patients not to speak during biomicroscopy and indirect ophthalmoscopy. I requested my patients wear masks until my county made it mandatory on July 8, 2020.
Related: Don’t forget to ask about CPAP usage
Because SARS-CoV-2 spreads primarily through droplets of saliva or discharge from the nose when an infected person talks, coughs, or sneezes, optometrists and staff are at high risk of exposure. COVID-19 is transmitted between persons who are within about 1.8 meters from each other. We are far closer than 1.8 m while performing slit lamp and indirect biomicroscopy.
Tear film exposure raises additional concerns. One study in 2003 reported the SARS coronavirus was detected in tears.2 Tear samples were obtained from 36 patients initially suspected to have SARS. Of those tested, 8 patients were considered probable SARS and confirmed by serology to have SARS, while 28 were SARS suspects based on symptoms and/or history of known exposure. Of the 8 probable SARS patients, tear samples from 3 patients (37.5 percent) yielded positive polymerase chain reaction (PCR) results. None of the SARS suspect patients had a positive PCR result.
I am not sure 37.5 percent would be compelling today. I found it hilarious that the authors noted, “Gloves were changed when collecting specimens in between patients to minimize risk of contamination”2. I remember when all I had to do was change gloves. Excuse me while I wash my hands for 20 seconds, careful to tilt them down, dry them with paper towel, which I hold in my hand while I touch the door handle, then throw it away and put on my mask. I bleach the chair, slitlamp table and headrest, the counters, the stand, the door knobs, light switches, and anything a human touched during the interaction, and then bleach the green flag outside the room door which I gleefully position to say, “Look, everyone, this room is clean”. But I digress.
Poll: What percentage of your pre-COVID patient base are you currently seeing?
A recent study of 17 COVID-19 patients found no evidence of the virus in tear samples tested using reverse‐transcription polymerase chain reaction (RT‐PCR) assay for the detection of SARS-CoV-2.3
A second study investigated the tear secretions of 30 confirmed coronavirus pneumonia patients. Tear and conjunctival secretions were collected twice during a 2- to 3-day period with disposable sampling swabs for reverse transcriptase PCR (RT‐PCR). Only one patient’s tears tested positive for SARS-CoV-2. He suffered conjunctivitis when the samples were taken, leading the authors to conclude that SARS‐CoV‐2 may be detected in the tears and conjunctival secretions in COVID-19 pneumonia patients with conjunctivitis.4
A third study of 43 patients with severe, confirmed cases of COVID-19 utilized RT-PCR to identify virus in the tear and conjunctiva. One patient has conjunctivitis. Three (7 percent) tear samples were positive for SARS-CoV-2, including the patient with conjunctivitis. All patients with positive tear RT-PCR results had positive nasopharyngeal RT-PCR results.5
Related: Committed to safety: One OD’s COVID-19 response
Tear samples were taken from 27 pediatric patients who tested positive using nasopharyngeal swabs for COVID-19 upon admission. Mild viral conjunctivitis was observed in 4 patients (15 percent). Conjunctival swab RT-PCR testing was positive in 3 patients (11 percent), 1 with symptomatic conjunctivitis, and 2 asymptomatic for conjunctivitis.6 Based on these studies, the transmission of SARS-CoV-2 is low, but caution should be taken in COVID-19 patients presenting with conjunctivitis. I am confident no optometrist needed to read this to know that he should not do tonometry on a COVID-19 patient with conjunctivitis.
Options for IOP measurement include Goldmann tonometry, Tonopen, noncontact tonometry (NCT), iCare, and transpalpebral tonometry. While certainly the standard for IOP measurement, the required proximity and the reuse of the tonometer tips make us nervous with COVID-19 exposures. Suggestions to reduce transmission risk include limiting IOP measurement to required cases such as recent postoperative patients, glaucoma patients, those taking topical steroids, or new patients where a baseline IOP is lacking. Multiuse tonometry devices should be cleaned per published guidelines prior to March 2020.7 Alternatively, disposable tips may be used, or it may be replaced with an alternative method.8
Tonopen
Tonopen applanation tonometry is based upon the Mackay Marg principle. The device requires anesthetic drops but does use disposable tip covers. This is advantageous when you would rather be an arm’s length away from the patient’s eye when performing IOP measurement compared to the 8 inches with Goldmann. Inter-instrument agreement and validity have been reportedly high, and its measurements correlate well with Goldmann tonometry.9 Lower IOP values in patients with IOP greater than 20 mm Hg on Goldmann have been reported.10
Related: Life with COVID-19 makes a new normal
Noncontact tonometry
The use of NCT has been questioned given the risk of spreading viral infection via tear dispersion. NCT uses a brief burst of pressurized air to applanate the cornea and measure IOP. Photographic analysis during performance of NCT found most eyes has some degree of tear film dehiscence and micro aerosol formation.11
A recent study evaluated aerosol measurements using NCT in 60 eyes of 30 subjects wearing masks and unmasked.12 Aerosol measurements were preformed using an 10000S+ air quality detector (Temtop). With repeated measurements, the aerosol particle numbers cumulatively increased. The density of the particle number was higher in unmasked subjects due to breathing compared to masked, but the difference was not significant. Investigators recommended staff wear medical goggles and mask while performing NCT. They further recommended a protective baffle should be placed between the technician and the patient.
Icare tonometry
The iCare tonometer is based on a rebound measuring principle to measure IOP. It does not require anesthetic drops and does not cause dispersion of tears. Its popularity prior to COVID-19 was patient response to the test, which was excellent. Its current popularity is more likely based on the device’s single use probes. I was surprised to note that even my local glaucoma specialist has been using iCare post-operatively since February 2020. Rebound tonometry has been found to correlate well with Goldmann IOP measurements, and also found to agree with Goldmann in eyes S/P corneal grafts.13 Home units are also available.
Transpalpebral scleral tonometry
Transpalpebral scleral tonometry is available. I am sure patients will consider this just as good as gas at the dentist. This device is based upon determining the acceleration of a freely falling rod as it rebounds against the tarsal plate of the eyelid through the sclera. While initially recommended for corneal disease such as ulcers, severe keratitis, and keratoconus, and postoperative corneal conditions,14 the Diaton (DevelopAll Inc., formerly BiCOM) tonometer’s applicability has expanded now that we would like to avoid touching the cornea while 8 inches from the patients face. Corneal biomechanics are less likely to influence measurement with this method, since there is no applanation of the cornea, which may be advantageous following keratorefractive surgery.15 No anesthetic is required, and patients look down when the test is performed.
Some comparisons of IOP measurement between examiners as well as to Goldmann have found no significant differences,16 while other studies have found poor agreement with Goldmann applanation tonometry, and voiced concern for its use in routine clinical practice.17,18 In the current climate where ODs want to provide care in the safest manner possible, evaluating IOP with a wider range of error while reducing infection risk may be more acceptable. There is a learning curve, but users have reported the online training is good.
I personally have increased my use of Tonopen and reduced my performance of Goldmann. I appreciate hand-held units, especially for my planned parade of in-car IOP checks should a second lockdown occur.
More by Dr. Swartz: Can azithromycin treat COVID-19?
References
1. McDermott G. Ophthalmologist Shares Experience Implementing Drive-Through IOP Checks Into Practice. Eyewire News. Available at: https://eyewire.news/articles/ophthalmologist-shares-experience-implementing-drive-through-iop-checks-into-practice/. Published 2020. Accessed 7/4/2020.
2. Loon SC, Teoh SC, Oon LL, Se-Thoe SY, Ling AE, Leo YS, Leong HN. The severe acute respiratory syndrome coronavirus in tears. Br J Ophthalmol. 2004;88(7):861-863.
3. Seah IYJ, Anderson DE, Kang AEZ, Wang L, Rao P, Young BE, Lye DC, Agrawal R. Assessing Viral Shedding and Infectivity of Tears in Coronavirus Disease 2019 (COVID-19) Patients. Ophthalmology. 2020;127(7):977-979.
4. Xia J, Tong J, Liu M, Shen Y, Guo D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J Med Virol. 2020;92(6):589-594.
5. Karimi S, Arabi A, Shahraki T, Safi S. Detection of severe acute respiratory syndrome Coronavirus-2 in the tears of patients with Coronavirus disease 2019. Eye. 2020;34(7):1220-1223.
6. Valente P IG, Federici M, Petroni S, Palma P, Cotugno N, De Ioris MA, Campana A, Buzzonetti L Ocular manifestations and viral shedding in tears of pediatric patients with coronavirus disease 2019: a preliminary report. Journal of AAPOS. 2020.05.02;20.
7. Seitzman GD, T. No Time for Tears. Ophthalmology. Available at: https://www.aaojournal.org/article/S0161-6420(20)30314-6/pdf. Accessed 7/3/2020.
8. Ng V, Tang G, Lai T, Tang E, Li K. Intraocular pressure measurement during COVID pandemic. Indian J Ophthalmol. 2020;68(5):950-951.
9. Schweier C, Hanson JV, Funk J, Töteberg-Harms M. Repeatability of intraocular pressure measurements with Icare PRO rebound, Tono-Pen AVIA, and Goldmann tonometers in sitting and reclining positions. BMC Ophthalmol. 2013;13:44.
10. Lester M, Mermoud A, Achache F, Roy S. New Tonopen XL: comparison with the Goldmann tonometer. Eye (Lond). 2001;15(Pt 1):52-58.
11. Britt JM, Clifton BC, Barnebey HS, Mills RP. Microaerosol Formation in Noncontact 'Air-Puff' Tonometry. Arch Ophthalmol. 1991;109(2):225-228.
12. Chunchun L YT, Zhangyan C, Aisun W, Xiaoqiong H, Yanyan C, Jia Q. Aerosol formation during non-contact “air-puff” tonometry and its significance for prevention of COVID 19. J Ex Ophthalmol. 2020(3).
13. Salvetat ML, Zeppieri M, Miani F, Tosoni C, Parisi L, Brusini P. Comparison of iCare tonometer and Goldmann applanation tonometry in normal corneas and in eyes with automated lamellar and penetrating keratoplasty. Eye (Lond). 2011;25(5):642-650.
14. Chakraborty AK, Majumder M, Sen S. Comparison of transpalpebral tonometer with Goldmann applanation tonometer. Taiwan J Ophthalmol. 2014;4(3):110-115.
15. Margarita Rozhdestvenskaya M, Dr. Alexey Dashevsky, Munchen, Prof. Dr.Ing. Dr. Habil. Konstantin Kotliar, FH Aachen and Campus Julich. Advantages of the extra corneal diatom tonometry in patients before and after photo refractive intervention Joint Event on 3rd Edition of International Conference on Eye and Vision & 2nd International Conference and Expo on Advanced Eye Care and Cataract. June 14-15, 2018 Rome, Italy.
16. Rozhdestvenskaya M DAaKK. Repeatability and inter-examiner reliability of non-corneal tonometry using Diaton. Int J Ophthalmic Pathol. 2019;8.
17. Doherty MD, Carrim ZI, O'Neill DP. Diaton tonometry: an assessment of validity and preference against Goldmann tonometry. Clin Exp Ophthalmol. 2012;40(4):e171-175.
18. Gunvant P, Miller B, Dalton K. Evaluation And Comparison Iop Estimates Obtained With Diaton Tonometer With Other Clinical Tonometers. IOVS. 2012;53(14):5077-5077.











Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.

















