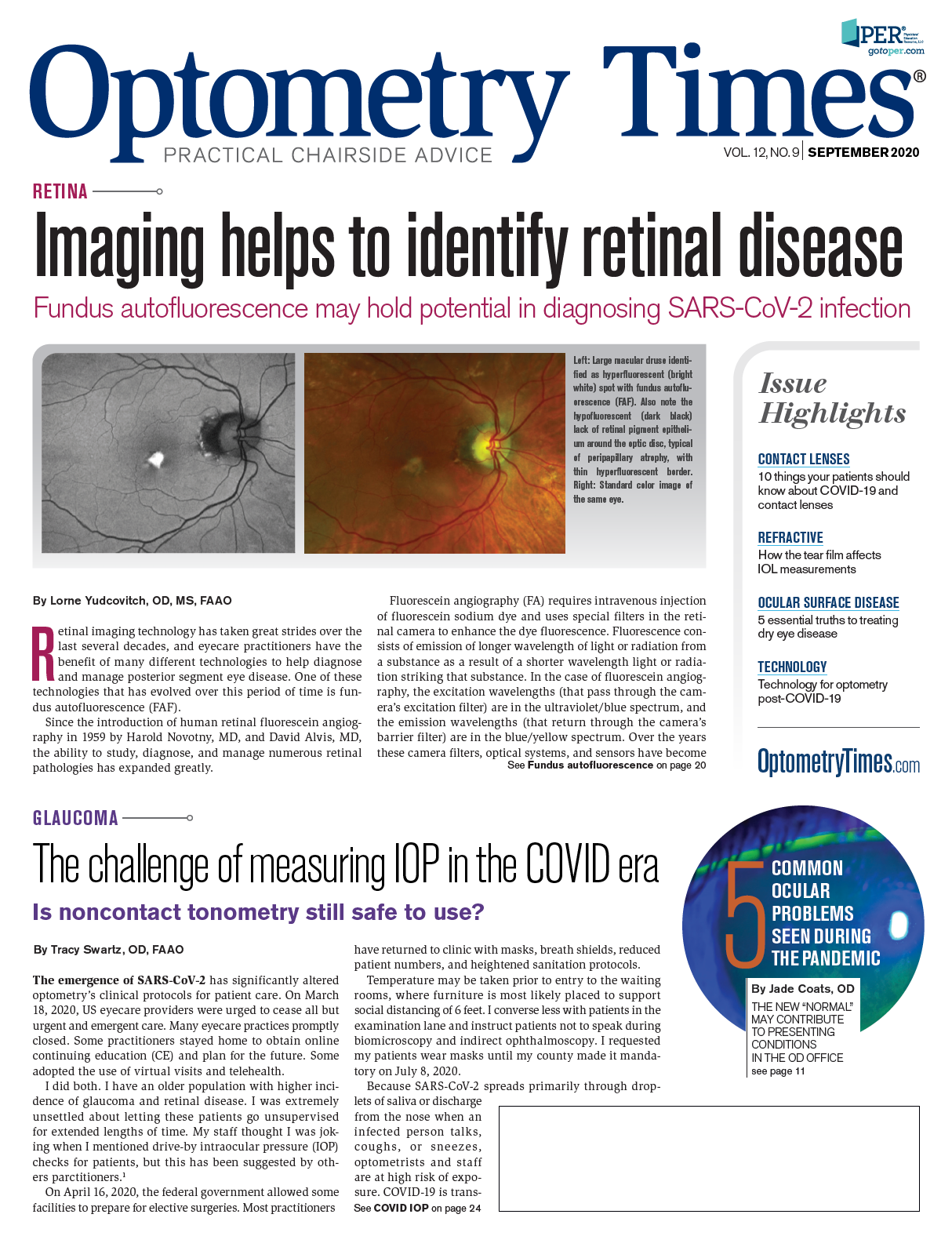
COVID-19 stole optometry’s 2020 thunder, but not all of it
Despite the pandemic, ODs have the ability to energize patients about eye health




As optometric practices modify operations to cope with COVID-19, ODs should not let current circumstances deter them from preparing for a post-pandemic office and, more importantly, from preparing patients for potential visual pitfalls.
I started 2020, the ophthalmic professions’ equivalency to a Jubilee or Golden era, lamenting optometric expectations. The realization that “we are in 2020” should have created euphoria only rivaled—well at least for me—by being named most read author of Optometry Times® (this can still happen!).
However, the year 2020 will not be remembered for the resemblance to perfect vision. Rather, it will be a reminder of how a pandemic can instill both fear and uncertainty in doctors and patients alike. As eyecare clinicians, we persist in doing our part to help patients. Current circumstances should not deter us from preparing for a post-pandemic office and, more importantly, from preparing patients for potential visual pitfalls.
Proaction and prevention
If you are a frequent reader of my prose, you will see a pattern in my thought process: proaction and prevention. As primary-care clinicians, ODs are supposed to guide patients into best practice by finding and treating disease early. As a patient advocate, you, me, and all in the practice should look for reasons to instill healthy ophthalmic habits.
Every patient is a dry eye patient until proven otherwise; you want to fight me on that? Inflammation and obstruction, the new hallmarks of dry eye, will not tolerate steroids and artificial tears for life. Patients will not change the overuse of digital devices. Furthermore, dry eye disease is not an old person disease but rather a human one.
Go read this study by Preeya Gupta, MD.1 She shows how early dry eye can present.
When is the last time you wrote an Rx for an immunomodulating/anti-inflammatory dry eye twice-a-day drop? (It should be like 1 minute ago!) Moreover, when did you last talk to your patients about blinking more, using lid scrubs or a moist-heat mask (that lasts longer than 10 minutes), and setting them up for a thermal pulsation or intense pulsed light (IPL) treatment? These should all be as common as prescribing contact lenses or discussing cataracts.
Reconsidering routines
Another area where the uncommon should become the routine is in ODs’ ability to diagnose vision disorders early enough to have a positive impact. When I think of inflammation on the cornea, I always reminisce to my problem-based learning ocular disease (PBLOD for short—maybe) from third-year optometry school. The goal was not to memorize the white-dot syndromes—if there is only 1 you can tell I didn’t listen too well—but rather, to look at the ramifications of the disease state and see how, as eye doctors, we can maintain good vision and reduce ocular damage.
Inflammation is arguably the root of all evil and yet a systemic necessity. Think of the pain that love can cause, and yet without it your life is not really fulfilled. Any corneal disease combined with inflammation is exacerbated. Managing any disease requires balancing, assessing risks, and doing our part to minimize them. Moreover, I would say it is also our duty to give patients sound advice to reduce potential damage.
Keratoconus, or rather the ectactic disorders, are a great example of this. Keratoconus, for years, has been diagnosed solely based on the inability to get a good retinoscopy. We all do retinoscopy, still, right? OK, most likely not—but your Spidey sense should tingle whenever a patient is incapable of 20/20 best-corrected visual acuity (BCVA), a big difference in correction between eyes, large changes to the refraction over years, or refractive inconsistency.
Good ol’ fashioned patient history
In this, our Jubilee year, I am skipping the VID for now. Most practices have a form of topography or tomography to evaluate surface curvature. However, good ol’ fashioned history can elucidate more diagnostic information, such as eye rubbing and family history. Neither of these is a great indicator alone for this disease; however, there is now a genetic test called AvaGen (Avellino). AvaGen is the first commercially available test that is non-invasive and examines 1,000 variants across 75 genes for keratoconus and over 70 transforming growth factors, beta-induced (TGFBI) mutations of the TGFBI gene for corneal dystrophies.2
It is one thing to tell a young patient or parent that they have keratoconus. It is another to give hope. Much like we do with early diagnosis of age-related macular degeneration (AMD) and glaucoma, intervention and lifestyle changes need to be made to reduce risk. With ectactic disorders, the 2016 approval of corneal collagen cross-linking (CXL), offered using the Photrexa Viscous, Photrexa, and the KXL system (Glaukos) is a game changer simply for being an option for patients. Managing this progressive disease takes optometry’s acumen with refractions and contact lenses, as well as our primary health advocacy. CXL is essentially the same as a photorefractive keratectomy (PRK) procedure, and the management is therefore similar. Some would argue the refractive result is the same—maintain good quality of vision, reduce further deterioration, and monitor for sequelae. The 1-2 punch of early detection and treatment options is in our wheelhouse.
Look, I get it. If someone had said to me that 2020 was going to be a year to forget I would have laughed in their face at a distance of less than 6 feet, without a mask. And yet here we are. As eyecare clinicians, we need to use this year to energize our patients for preparedness, early detection, and concomitant morbidities. Much like dry eye, keratoconus is an example of ways to integrate that PBLOD into your practice—just do it from a safe distance.
Reference
1. Gupta PK, Stevens MN, Kashyap N, Priestley Y. Prevalence of Meibomian Gland Atrophy in a Pediatric Population. Cornea. 2018;37(4):426-430.
2. New Avagen genetic test. Avellino. Available at: https:// www.avellino.com/en/products/avagen-test/. Accessed: 8/31/2020.











Newsletter
Want more insights like this? Subscribe to Optometry Times and get clinical pearls and practice tips delivered straight to your inbox.

















